


IRREGULAR ASTIGMATISM 2
Irregular Astigmatism, Part 2
This second article of a three-part series discusses when to prescribe large corneal and scleral GP lenses to manage irregular astigmatism.
By Susan Kovacich, OD
Last month, I addressed using small-diameter, steep corneal GP lenses to manage irregular astigmatism caused by small, centrally located keratoconic cones. But what design should you choose when the keratoconic cone is larger (oval cone, Figure 1), very large (globus cone), or is located away from the visual axis (Figure 2)? What is the best way to manage other causes of irregular astigmatism that result from other conditions, including corneal surgery (Figure 3) and trauma?
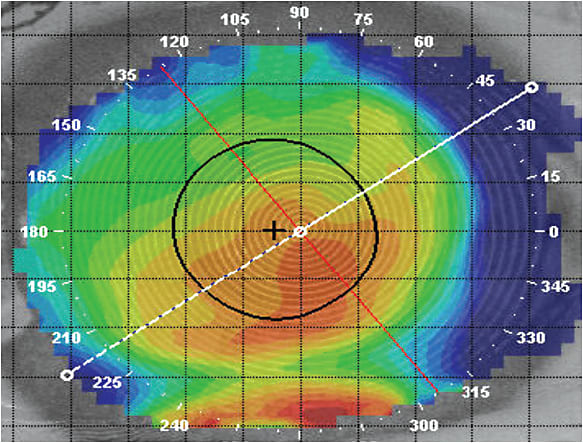
Figure 1. Oval cone.
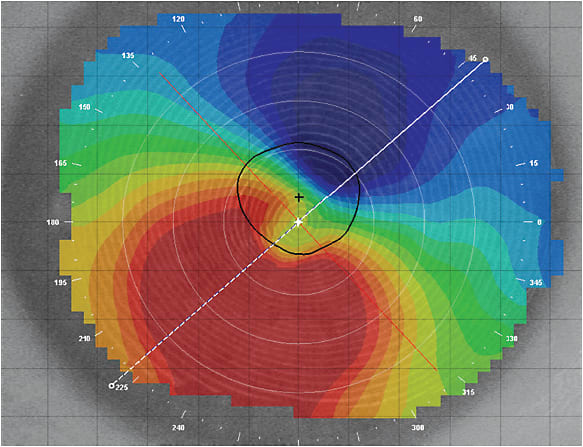
Figure 2. Large inferior globus cone.
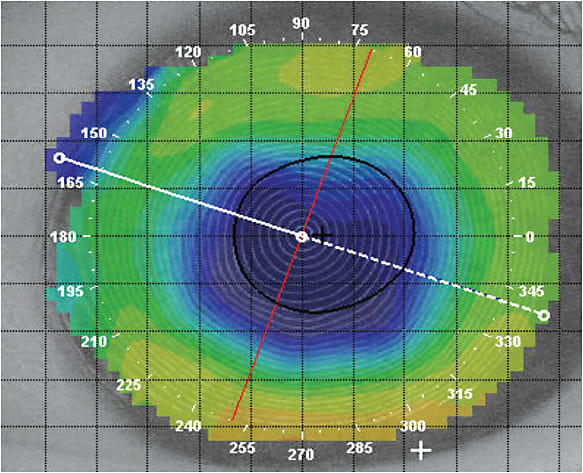
Figure 3. Status post-radial keratotomy.
Small Versus Large Corneal GPs
As a corneal contact lens will center toward the steepest area of the cornea, irregular astigmatism that is off-axis often cannot be adequately managed with a small GP lens. When the lens is displaced, the visual axis is no longer aligned with the optical center of the lens. With severe displacement, patients may be viewing through the peripheral curves or the edge of a small GP lens.
Large-diameter corneal GP lenses move less on the eye and therefore generate less tear exchange; higher-oxygen-permeable (higher-Dk) GP materials have allowed manufacturers to produce large-diameter or intralimbal corneal GP lenses (10mm to 12.5mm, Figure 4) with larger optical zone diameters that do not compromise corneal health. The weight of these larger lenses is distributed over the peripheral cornea, allowing them to center better compared to small-diameter GP lenses. If lens displacement does occur, the larger optical zones allow patients to view through the proper portion of the lens and maintain better visual acuity. These lenses also tend to be more comfortable as there is less lens interaction with the upper lid (Bennett et al, 2013). As with smaller specialty GP lens designs, many of these lenses are also available with quadrant-specific peripheral designs that can help the lenses better align with irregular corneas and provide suitable edge lift.
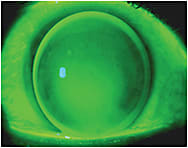
Figure 4. A large-diameter corneal lens.
Fitting a keratoconus patient with a large-diameter corneal lens is similar to fitting a smaller GP lens for keratoconus; three-point touch with feather apical touch of the cone is considered appropriate. Corneal irregularities due to other pathologies, surgery, or trauma should be fit to allow for adequate tear exchange, good corneal clearance, and appropriate edge lift with no bubbles under the lens. It is important to note that when fitting a corneal transplant with a large-diameter corneal GP lens, the optical zone diameter should be larger than the graft to vault the host-graft interface and protect it from mechanical trauma and possible rejection (Louie et al, 2013).
Reverse Geometry Lenses
Normal corneas have a prolate shape, but after refractive corneal surgery for myopia, the central ablation zone produces a central flatter corneal region surrounded by an area of steeper peripheral cornea (Figure 3). A sunken corneal transplant graft may have a similar shape. If there is post-surgical residual irregular astigmatism that requires a GP lens, this now oblate cornea is often better fit with a reverse geometry design to prevent excessive central corneal clearance with disproportionate midperipheral bearing.
Attaining an alignment fit with minimal vault in the central flat zone while not impinging on the steeper midperipheral cornea can often only be achieved with a lens that has a flat central base curve and a secondary “reverse curve” that is steeper compared to the base curve (Louie et al, 2013). The profile of a reverse geometry lens resembles a plateau; the earliest reverse geometry lenses were designed to manage radial keratotomy (RK) patients and were called “plateau lenses.”
Computer-guided lathes made the manufacturing of these advanced GP designs possible. Reverse geometry designs are often designated as “post-surgical” or “oblate” lenses; certain designs have also revolutionized corneal reshaping. They are available in large-diameter corneal GP, scleral, and hybrid lenses.
Choosing Between Corneal GP Lenses and Scleral Lenses
It would be helpful if there was a way to know when to select a corneal GP versus a scleral lens to save chair time, but how do you know when the corneal irregularity is too severe for a corneal GP lens? Caroline and André (2015) have suggested that a change in elevation greater than 350 microns (using the topographical elevation map) between the steepest and flattest portion of the cornea along the meridian of greatest elevation difference would be too pronounced to be fit successfully with a corneal GP.
As an example, from the axial power topography map in Figure 5, we initially expected that a large corneal GP would be able to adequately fit this keratoconic cornea. After several frustrating attempts to eliminate bubbles under the lens, we finally selected a scleral lens and fit the patient successfully. A later analysis of the elevation map of this cornea (Figure 6) revealed a height difference of 423 microns, which indicated that utilizing a corneal lens would be problematic. Knowing the height differential information reported by Caroline and André could have prevented aggravation for both patient and practitioner.
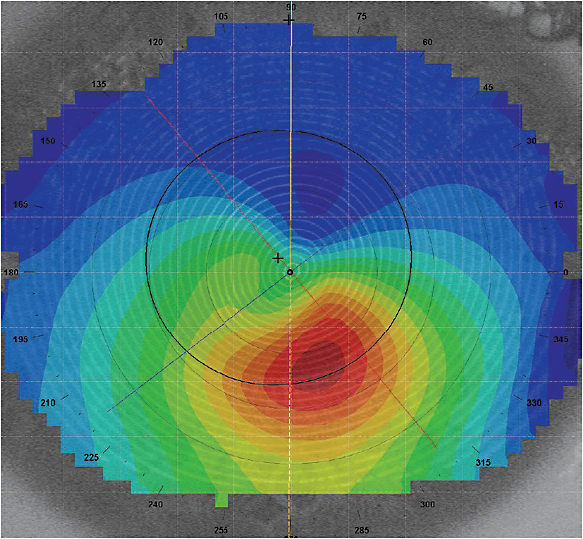
Figure 5. Axial display.
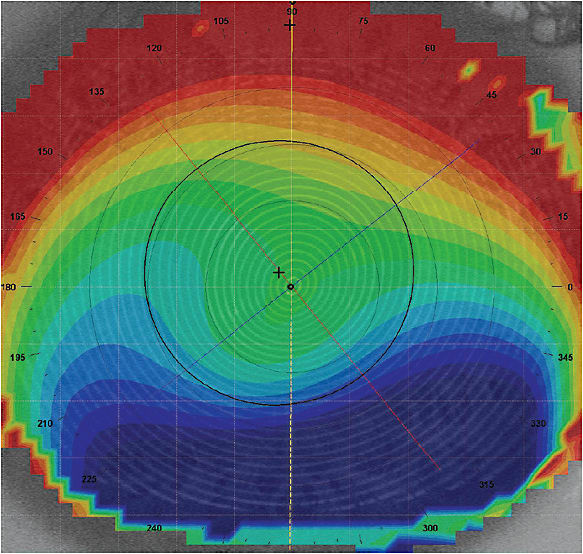
Figure 6. Elevation display of same cornea as Figure 5.
Scleral Lenses: Go Big, or Go…Bigger
As discussed previously, large-diameter corneal GP lenses have limitations in fitting extremely irregular corneas that result from conditions such as keratoconus, pellucid marginal degeneration (Figure 7), irregular corneal grafts (Figure 8), and Salzmann’s nodular degeneration (Figure 9). Fitting these corneas with large-diameter corneal lenses often results in a substandard fitting relationship, poor comfort, and poor vision. Until the last decade, an irregular cornea that could no longer be managed with a specialty corneal lens would likely progress to corneal transplantation.
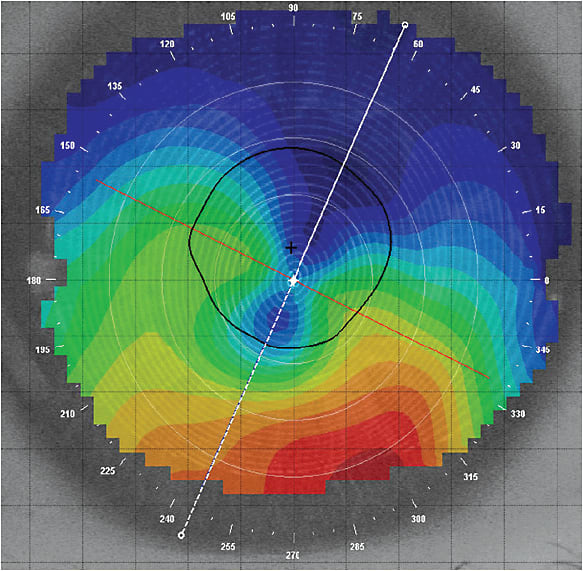
Figure 7. Pellucid marginal degeneration.
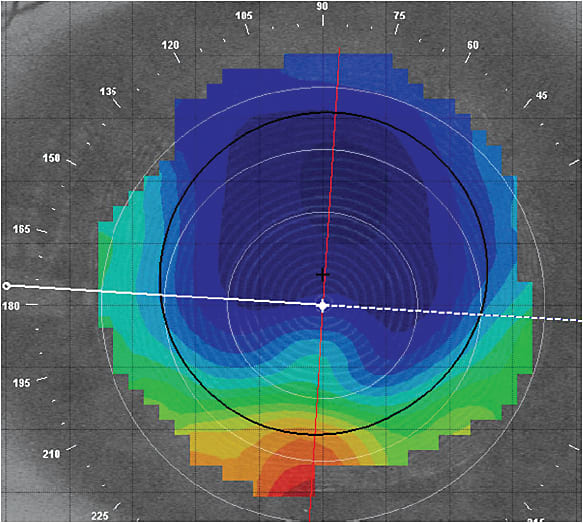
Figure 8. Irregular corneal graft.
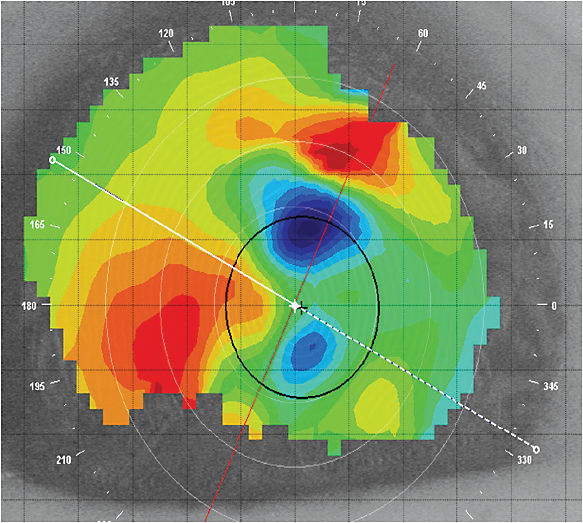
Figure 9. Salzmann’s nodular degeneration.
Once again, the combination of high-Dk materials and computer-generated designs made extremely large lenses, such as scleral lenses, a viable option for managing not only irregular astigmatism, but other refractive needs and ocular pathologies as well. Contact lens fitters have become more comfortable with these large lenses; in 2015, for the first time in the United States, scleral lenses were fit more than GP multifocal or toric lenses were. As a result, scleral lenses now represent 3% of the total U.S. contact lens market in which 9% are GP lenses, and this percentage is expected to continue growing (Nichols, 2016).
Scleral lenses land on the sclera and completely vault the cornea, holding a tear reservoir under the lens. Mini-scleral lenses are 15mm to 18mm in overall diameter or up to 6mm larger than the horizontal visible iris diameter (HVID), and full scleral lenses are 18mm to 25mm in overall diameter or ≥ 6mm larger than the HVID (van der Worp, 2015; DeNaeyer et al, 2013). Scleral lenses were the first contact lenses designed and fit on human eyes; early sclerals consisted of glass blown or ground glass shells. Not only were these lenses difficult to manufacture and reproduce, the glass was impermeable to gas/oxygen exchange. Also, the lenses were molded to the shape of the eye, so metabolic waste and toxins that would build up under the lenses made them unwearable after a few hours. This is obviously not the case with properly fit modern scleral designs (van der Worp, 2015; DeNaeyer et al, 2013).
Benefits of Scleral Lenses Because scleral lenses are very large (Figure 10), they have minimal movement and fit well under the eyelids, making a well-fit scleral lens comfortable to wear. As noted previously, they vault completely over the cornea; any corneal touch will usually register as lens awareness or discomfort. These large lenses are also extremely stable and do not dislocate on irregular corneas as corneal GPs can. As scleral lenses can vault over extremely distorted corneas, this modality may be the only contact lens option for patients who have high amounts of irregular astigmatism.

Figure 10. Scleral lens in situ.
Anatomy of a Scleral Lens All scleral lenses have an optical zone, a transition zone, and a landing zone or haptic. The optical zone can be spherical or aspheric, and a toric front surface can be used to correct residual astigmatism. The post-optic zone bridges the optical zone to the transition zone.
The transition zone is also called the midperipheral or limbal zone. This zone determines the sagittal height of the scleral lens. If an oblate scleral lens design is required, the reverse curve is in this location. Care must be taken to vault the limbus to maintain good corneal health.
The landing (haptic/scleral) zone is the portion of the lens that bears on the sclera. Success with scleral lenses depends on how well the landing zone is fit. Because the sclera angles tangentially away from the cornea, some lens designs have landing zones designed to mimic this shape. Landing zones and peripheral curves can be steepened and flattened as needed (van der Worp, 2015; DeNaeyer et al, 2013).
Fitting Scleral Lenses
When fitting scleral lenses, the parameters to consider include overall diameter, clearance (corneal, peripheral, and limbal), landing zone fit, lens edge lift, and whether an asymmetric-back-surface design (toric haptic) is needed. Diagnostic fitting sets are generally used to fit these lenses; empirical fitting is not recommended at this time unless a practitioner has one of the newer corneo-scleral topographers that can provide ocular shape data beyond the cornea.
Both the manufacturers’ guidelines and fitting consultants are valuable resources for fitting these lenses. Anterior segment optical coherence tomography (OCT) can provide important information for troubleshooting difficult fits. OCT images and digital images taken with a slit lamp camera or cell phone also can provide fitting consultants with helpful data for making modifications to improve fitting (van der Worp, 2015; DeNaeyer et al, 2013).
Diameter A scleral lens should rest on the scleral surface, while creating adequate corneal and limbal clearance. Choose the initial diameter based on the fitting guide. Corneas that have greater differences in elevation will likely require larger scleral lenses.
Lens diameter can be changed to improve the fit. The optical zone diameter of these lenses is often a fixed parameter; if a larger optical zone is needed, fitting a larger diameter may be necessary (van der Worp, 2015; DeNaeyer et al, 2013).
Clearance (Corneal, Peripheral, Limbal) A scleral lens should clear the cornea and limbus and have no areas of bearing. Scleral lenses are typically fit using sagittal height in microns; a greater sagittal height will increase the clearance of the lens.
Corneal Clearance Scleral lenses tend to settle or sink into the conjunctiva over the course of the wearing day, so it is important to account for that when evaluating the initial corneal clearance. Lenses tend to settle 100 to 200 microns with wear; waiting 20 to 30 minutes to evaluate the lens is helpful to determine how much clearance remains (van der Worp, 2015; DeNaeyer et al, 2013).
Full settling of the lens can take several hours to occur. A range of 100 to 300 microns of corneal clearance is acceptable after settling. A thick optical system created by excessive clearance (500 microns or more) may affect visual acuity. A minimum of 100 microns of central corneal clearance is the goal after scleral lens settling of 8 hours or more (van der Worp, 2015; DeNaeyer et al, 2013).
Use the thickness of the scleral lens as the gauge for evaluating the corneal clearance or tear lens vault when fitting irregular corneas. This is a known value for each type of scleral lens, whereas irregular corneas can vary in thickness, so the lens thickness makes a better reference when evaluating how much clearance is behind the lens in microns. When fitting a healthy cornea with scleral lenses, the corneal thickness can also be used to determine the corneal vault.
To make the tear lens more visible for evaluation, instill a drop of sodium fluorescein in the nonpreserved saline that fills the bowl of the scleral lens. Following fluorescein instillation, vault is best evaluated using an optic section with white light (Figure 11); it is more difficult to evaluate with cobalt blue light. Adequate corneal clearance is demonstrated by an even pattern of fluorescein with no areas of bearing in primary position with a wide beam (van der Worp, 2015; DeNaeyer et al, 2013).

Figure 11. Central vault.
Limbal Clearance The scleral lens should align with the limbus and avoid any bearing on this delicate region, with the lens landing 0.5mm to 1.0mm beyond the limbus. Fluorescein visualized over the limbus is indicative of clearance in this region (van der Worp, 2015; DeNaeyer et al, 2013).
Peripheral Corneal Clearance Peripheral corneal touch is also not acceptable. If the central clearance is adequate but the peripheral clearance is not, you may need a larger-diameter lens, which will increase the sagittal height of the lens provided that the optical zone remains the same. A reverse geometry design can be used when indicated (oblate cornea) (van der Worp, 2015; DeNaeyer et al, 2013).
Landing Zone Fit The landing zone should align with the sclera so that the weight of the lens is distributed evenly over the conjunctival tissue that overlies the sclera. Conjunctival vasculature should be patent, with no areas of compression or blanching of the blood vessels. Excessive bearing in the inner portion of the landing zone is caused by a flat landing zone; excessive bearing on the outer portion of the landing zone is caused by a steep landing zone (van der Worp, 2015; DeNaeyer et al, 2013).
Lens Edge Fit As with a corneal GP lens, some edge lift is necessary for a good scleral fit. Too much edge lift can register as lens awareness; too little edge lift can dig into the conjunctiva and cause impingement. An excessively tight edge will result in lens seal-off and decreased wearing time due to discomfort. If the lens edge is a parameter that cannot be modified independently, the landing zone angle may have to be changed (van der Worp, 2015; DeNaeyer et al, 2013).
Asymmetric-Back-Surface Design (Toric-Back-Surface Haptic) Many scleral lenses have spherical-back-surface haptic designs. Measurements of the anterior ocular surface have improved in recent years, revealing that the sclera has a nonrotationally symmetric (or asymmetric) structure.
To distribute the pressure of the haptic more equally over this surface, asymmetric-back-surface designs or toric scleral lens designs have been created. These designs can improve comfort and fit. If a lens is found to bear too much on the sclera in one meridian and to stand off in the meridian 90° away, a toric scleral design is indicated. Toric designs may also help reduce unwanted debris that can collect in the tear reservoir of scleral lenses.
Larger scleral lenses may require this design more compared to smaller scleral lenses. Back-surface toric lenses may also make it unnecessary to ballast front-surface toric lenses. Quadrant-specific designs are also available from some manufacturers.
Power Determination Finally, after the proper lens fit is selected and allowed to settle for 20 to 30 minutes, perform an over-refraction to calculate the proper lens power (van der Worp, 2015; DeNaeyer et al, 2013).
Scleral Lens Application, Removal, and Care
The bowl of the scleral lens should be completely filled with sterile saline until there is a positive meniscus to facilitate placement on the eye without bubbles. Multipurpose solutions are considered too toxic for use with scleral lenses, and nonpreserved multi-use saline bottles are not sterile after opening. Some practitioners use 0.9% inhalation saline off-label to fill scleral lenses; however, a U.S. Food and Drug Administration (FDA)-approved saline for use with scleral lenses has just been released to the market.
A large scleral lens filled with fluid is top heavy and difficult to manage; many patients use a large plunger with a hole (to prevent suction) to aid in positioning the lens for application. Some patients can master a two-finger or three-finger tripod technique. Patients must position their head parallel to the floor; tucking in the chin helps to position the face properly.
Scleral lens removal generally requires a plunger with no hole to provide suction. After making sure that there is a lens on the eye, patients place the plunger on the lower third of the lens and lift it up and out of the eye.
Cleaning and storage of scleral lenses can be a challenge; peroxide disinfection solutions are often used if the lenses can fit in the baskets of the lens cases used with these systems (van der Worp, 2015; DeNaeyer et al, 2013).
Scleral Lens Challenges
Although scleral lenses are sometimes the only lens modality that can manage severe irregular astigmatism, they do have their challenges. First, as mentioned previously, scleral lenses currently require fitting with diagnostic sets except for practitioners who have one of the newer corneo-scleral topographers. Next, practitioners need to have some basic training to become comfortable with this modality; workshops can be a wonderful way to obtain critical skills and confidence. In addition, just as practitioners need to become capable with scleral lens application and removal instruction, so do their technical staff. Lastly, patients (or their caregivers) need to have the desire and ability to handle these large lenses.
Practitioners also need to adjust their fees for fitting scleral lenses, which typically require more time compared to fitting conventional GP lenses. Fitting scleral lenses can be intimidating at first, but they can literally be life changing for patients who have advanced irregular astigmatism. Being able to offer this modality to patients, or finding a colleague who can, is an important service that practitioners can provide to their patients.
Still to Come
The final part of this three-part series will appear in the June issue. It will focus on managing irregular astigmatism using piggyback lens systems, hybrid lenses, and specialty soft lenses. CLS
For references, please visit www.clspectrum.com/references and click on document #246.

| Dr. Kovacich graduated from Indiana University (IU) School of Optometry and completed a hospital-based residency at the St. Louis VAMC. After practicing for 10 years, she returned to IU and is an associate clinical professor in the Cornea and Contact Lens Service. She was a consultant to Alcon and has received travel funding from Alcon, Bausch + Lomb, Johnson & Johnson Vision Care, Inc., and CooperVision. |