


CONTACT LENS ADVANCEMENTS
The Here, Now, and to Be of Contact Lenses
A look at materials and designs for the 21st century and beyond.
By Cecilia Chao, MOptom, PhD, & Kathryn Richdale, OD, PhD
It’s an exciting time in the field of contact lenses. No longer are they considered just a means of correcting refractive error. These medical devices may also be used to deliver ocular pharmaceuticals, slow the progression of myopia, monitor ocular and systemic diseases, and help guard against infection, among other things.
The U.S. Food and Drug Administration (FDA) has cleared the use of contact lenses as a correction for refractive error or as bandage lenses for anterior segment problems. But other indications for contact lenses are approved outside of the United States and are in various stages of research and development.
There are more than 40 million contact lens wearers in the United States alone (Cope et al, 2015; Wagner et al, 2011). While this is a large number of people utilizing a prescription medical device, it represents only about 13% of the total U.S. population. Non-refractive indications for contact lenses could lead to a major expansion of contact lens prescribing.
This article provides a glimpse into new contact lens designs and materials in development to give readers an idea of the potential contact lens practice in the 21st century and beyond.
Contact Lenses and Therapeutics
Topical ocular pharmaceuticals are the primary treatment for glaucoma, dry eye disease, and ocular surface inflammation or infection. Ocular medications have clear benefits over systemic drugs as they provide treatment directly to the affected site and thus lower the rate of systemic complications.
Unfortunately, there are still limitations to the use of topical ophthalmic drugs. Only about 1% to 7% of topical medications reach the target tissue at an effective therapeutic dose due to tear dilution, variable penetration, non-specific absorption, and drainage or overflow from the eye (Ghate and Edelhauser, 2008; Hsu et al, 2014; Phan et al, 2014). This can lead to subtherapeutic levels of antibiotics and to challenges in maintaining a consistent intraocular pressure (IOP), for example. It also necessitates multiple daily dosing for many drugs.
The concept of using a contact lens for drug delivery was first proposed by Sedlavek in 1965. A contact lens could provide a drug reserve in the post-lens tear film and thus prolong the contact time on the ocular surface (Li et al., 2006). Contact lenses have also been used to support the transfer of limbal stem cells to rehabilitate the ocular surface (Bobba and DiGirolamo, 2016). The use of contact lenses as a drug or stem cell delivery system could improve corneal health, reduce fluctuations in treatment effects, and reduce or eliminate multiple drug dosing requirements.
Current Development The use of a contact lens to deliver drugs was first undertaken by simply soaking a commercial contact lens in an ocular medication. This method has been used with antibiotic (Jain, 1988), anti-inflammatory (Jain and Batra, 1979), anesthetic (Hrazdirová et al, 1990), and glaucoma (North, 1971) medications (see also review by Hui and Willcox, 2016).
Soaked lenses generally release an initial burst of drug followed by a quick drop off in concentration. The longest duration of drug release from soaking studies varies from minutes to a few hours, depending on the drug and lens material properties (Carvalho et al, 2015; Hsu et al, 2014). While preliminary studies indicate good efficacy for increasing ocular surface retention, the lack of controlled release limits the use of this method.
Thanks to improvement in technology, there are several new methods being explored to provide a longer and more controlled release of drugs from contact lenses. These include—but are not limited to—molecular imprinting, nanoparticles, and vitamin E barriers.
Molecular imprinting creates “cavities” in a polymer that function similar to a lock and key to bind and release a drug from a contact lens material (Hsu et al, 2014). Molecular imprinting can carry up to 300 times more drug and can extend the release duration by up to 50 times longer than that of soaked commercial lenses (Alvarez-Lorenzo et al, 2006; Hiratani et al, 2005; Tieppo et al, 2012; Venkatesh et al, 2007).
Molecular imprinting has been used with both hydrogel and silicone hydrogel contact lens materials and a variety of drugs including timolol, prednisolone acetate, ketotifen, ciprofloxacin, and atropine (Lasowski and Sheardown, 2016; Ali et al, 2007; Alvarez-Lorenzo et al, 2006; Hiratani et al, 2002; Malaekeh-Nikouei et al, 2012). Unfortunately, research using this method has reported alterations of certain contact lens parameters (Hsu et al, 2014).
Nanoparticles may also be used to encapsulate a drug to achieve a slower, more controlled release. Nanoparticles have been tested in laboratory and animal studies with antibiotics, antifungals, anesthetics, and others. Some of the challenges of this delivery include the increased thickness of the nanoparticle gels (Kapoor and Chauhan, 2008) and inconsistent drug release (Gulsen and Chauhan, 2005), including potential release of drug while in storage. Researchers have attempted to address the latter by the use of temperature-sensitive nanoparticles (Hsu et al, 2014; Jung and Chauhan, 2012).
Vitamin E barriers have also been explored to increase the duration of drug diffusion from contact lenses. The vitamin E molecule acts as a diffusion barrier, but is biocompatible, oxygen soluble, and also adds ultraviolet blocking properties (Kim et al, 2010; Peng et al, 2011). This has increased drug uptake and release duration compared to soaked-contact lenses and standard eye drops with in vitro and animal models (Danion et al, 2007; Xu et al, 2010). However, due to the fact that vitamin E is hydrophobic, the release duration varies for hydrophilic, hydrophobic, and amphiphilic drugs (Hsu et al, 2014).
Looking Ahead Table 1 provides an overview of the development of drug delivery contact lenses in the treatment of ocular disease (Hsu et al, 2014; Hui et al, 2016). To date, only a few animal and human studies using these drug delivery contact lenses have demonstrated efficacy.
| Drug Category | Methods | Research Testing |
|---|---|---|
| Anti-glaucoma | Soaking | Human |
| Vitamin E coating | Animal | |
| Molecular imprinting | Animal | |
| Nanoparticles | Animal | |
| Antibiotic | Soaking | Human |
| Molecular imprinting | Animal | |
| Nanoparticles | In vitro | |
| Anti-allergy | Molecular imprinting | Animal |
| Anesthesia | Soaking | Human |
| Vitamin E coating | In vitro | |
| Nanoparticles | In vitro | |
| Anti-inflammatory | Soaking | Human |
| Vitamin E coating | In vitro | |
| Molecular imprinting | In vitro | |
| Nanoparticles | In vitro | |
| Anti-myopia | Molecular imprinting | In vitro |
One of the challenges facing drug delivery technologies is that they may affect important material properties of the lens, such as oxygen transmissibility, modulus, or transparency (Jung et al, 2013). Additionally, for drug delivery contact lenses to be truly useful in practice, they would ideally provide a controlled, sustained release of drug over at least one week. One of the regulatory challenges facing these treatments would be FDA approval of a “combination product” (both a device and drug or biologic).
Contact lenses coated with epithelial stem cells have been successfully used in a limited number of limbal stem cell deficiency and post-graft patients with success rates similar to other limbal stem cell transplant techniques (Bobba and DiGirolamo, 2015). But further research is needed to understand how various material properties can better support cell detachment from the lens and adhesion and proliferation on the damaged cornea.
Although there are still significant challenges ahead, the potential benefits of developing stem cell and drug delivery contact lenses are significant in that they could significantly improve corneal health and provide better management of both chronic and acute diseases.
Anti-Microbial Contact Lenses
Contact lens wear is one of the major risk factors for corneal infiltrative and inflammatory events, including the most severe—microbial keratitis (MK) (Stapleton et al, 2013). This is, in part, due to the fact that a contact lens acts as a reservoir to transport microorganisms to the ocular surface. Pseudomonas aeruginosa, Serratia marcescens, and Staphylococcus aureus (coagulase-negative staphylococci [CNS]) are the most commonly isolated bacteria from MK (Dutta and Willcox, 2014; Green et al, 2008; Stapleton et al, 2013). Other gram-negative and gram-positive bacteria have been cultured from contact lens-associated red eye (CLARE) and contact lens peripheral ulcer (CLPU) cases. In addition, “non-infectious” or “sterile” keratitis may actually be due to exotoxins of dead bacteria and biofilms.
Currently, the primary antimicrobial strategy is via the use of contact lens care solutions to “disinfect” contact lenses prior to reuse. Unfortunately, no lens care solution is able to fully disinfect contact lenses without also being toxic to the ocular surface. This is further compounded by patients’ poor lens wear and care behaviors, such as rinsing contact lenses with water or “topping off” (reusing) lens care solution (Wagner et al, 2011). Because of this, reusable contact lenses and lens cases routinely show high levels of bacterial contamination (Larkin et al, 1990). The idea behind an antimicrobial contact lens is to further reduce the number of viable bacteria presented to the ocular surface with contact lens wear.
Current Development Antimicrobial products can work by inhibiting the microbial cell wall, protein or nucleic acid synthesis, or production of metabolites. This can be achieved by a number of techniques including incorporation of metals, mineral elements, non-steroidal anti-inflammatory drugs (NSAIDs), and antimicrobial peptides (AMPs).
Silver has been tried as an antimicrobial agent in several medical areas, including endotracheal tubes and urinary catheters (Lansdown, 2006). Silver has many mechanisms of action, making resistance less likely; it also shows anti-fungal activity (Dallas et al, 2011; Dias et al, 2006). Unfortunately, the antimicrobial efficacy of silver can be reduced by human fluids such as plasma and tears (Rai et al, 2009). Furthermore, silver can have toxic effects in large doses or with continuous use, including a blackening of exposed tissues (Dutta and Willcox, 2014). Other metals, such as copper, zinc, nickel, and titanium, are being explored for medical use, but concerns have been raised regarding their effect on human cells (Dutta and Willcox, 2014).
NSAIDs have antimicrobial properties and can inhibit bacterial adhesion and biofilm formation (Kakisu et al, 2013). But, the negative potential effects of long-term NSAID use, including delayed wound healing, may limit its usefulness in the eye (Hsu et al, 2014).
Selenium compounds can produce superoxide and hydrogen peroxide to damage bacterial cells, but they do not harm mammalian cells (Palace et al, 2004). Organo-selenium compounds bound to hydrogel or silicone hydrogel contact lenses significantly reduced the adhesion of both gram-positive and gram-negative bacteria (Tran et al, 2009) and had no adverse effects on the ocular surface after two months of extended wear in an animal model (Mathews et al, 2006). The efficacy and safety of this mechanism has not been investigated in clinical trials.
Quorum sensing inhibitors block bacterial cell-to-cell communication systems and, by doing so, inhibit bacterial adhesion and formation of biofilms (Baveja et al, 2004). This method may prove more advantageous compared to traditional antimicrobials, which can lead to an increase in the volume of dead bacteria and have other detrimental effects on the ocular surface.
One of these synthetic compounds, fimbrolide, reduced adhesion to contact lenses of the most common bacteria associated with MK and showed no adverse events either in animal studies or in a 24-hour human trial (Zhu et al, 2008). Fimbrolide also did not alter key contact lens properties (Baveja et al, 2004).
Similarly, other non-bactericidal agents may help reduce biofilm formation and ultimately decrease infiltrative or infectious events. These types of agents, such as polyethylene glycol (PEG), would still need to be used with active bacteriostatic and bactericidal agents, but could reduce both protein deposition and microbial adhesion (Salwiczek et al, 2014).
Recently, AMPs were identified as having broad-spectrum activity against bacteria, fungi, protozoa, virus, and parasites (Dutta et al, 2013). AMPs are part of the innate immune response and act by destabilizing the membrane of microorganisms without damaging human cells (Willcox et al, 2008). There is some concern that the use of natural AMPs may result in development of microbial resistance to an innate immune response; thus, synthetic AMPs have been developed.
One that has undergone the most testing to date is melimine, a combination of melittin (from bee venom) and protamine (from salmon sperm). Melimine is effective against both gram-positive and gram-negative bacteria as well as fungi and Acanthamoeba (Cole et al, 2010; Dutta et al, 2013). Melimine-coated contact lenses reduced the severity of CLARE and CLPU in animal models (Cole et al, 2010). It was recently tested in a one-day randomized clinical trial with 17 adults and showed good acceptance and physiology except for a small increase in corneal staining compared to control lenses (Dutta et al, 2014).
Looking Ahead The development of antimicrobial contact lenses is still at an early stage. To date, there have been only a few small clinical trials. Following initial proof-of-concept and safety studies, large-scale trials will be needed to demonstrate efficacy.
One of the challenges facing clearance of these lenses is that the incidence of infiltrative and infectious events is relatively small. Large extended wear clinical trials may be cost-prohibitive, and thus post-market designs will likely be necessary to fully understand the effect that these devices have on the incidence and severity of contact lens complications.
Further complicating clearances will be potential interactions with different contact lens care products. That being said, with an expected increase in the total number of patients using contact lenses—both due to the aforementioned new indications and the growing prevalence of myopia—it is a challenge worth undertaking.
Myopia Control Contact Lenses
More than 40% of the U.S. population is myopic, and the incidence continues to increase worldwide (Lin et al, 1996; Vitale et al, 2008; Wang et al, 2009). While long considered a “nuisance” requiring correction with glasses, contact lenses, or surgery, there is now clear evidence that even low levels of myopia are associated with increased risk of glaucoma, retinal detachment, and myopic maculopathy (Flitcroft, 2012). Higher levels of myopia carry increasingly greater risks for comorbid eye disease. Fortunately, both animal and human research studies provide strong evidence of the ability of certain contact lens designs to slow the progression of myopia.
Current Development Soft multifocal contact lenses and orthokeratology are the two contact lens options being studied for myopia control. Both are purported to work by creating myopic defocus (positive lower- or higher-order aberrations) on the retina (Flitcroft, 2012).
Multiple studies have demonstrated that various soft multifocal contact lens designs can slow the progression of myopia (Cheng et al, 2015; Lin et al, 1996; Sankaridurg et al, 2011). The two randomized clinical trials published to date found that axial elongation was slowed by about 40% over the course of a year, although some questions remain regarding the long-term ability of a single lens design to maintain a significant myopia control effect (Cheng et al, 2015; Lam et al, 2014). These studies also demonstrated that children as young as age 7 years old were able to safely wear contact lenses with proper education and follow-up care. Visual acuity may be expected to be compromised with multifocal designs, especially with higher plus additions, but studies report about 20/25 or better Snellen-equivalent acuities under high-contrast, high-illumination settings (Cheng et al, 2015; Lam et al, 2014; Sankaridurg et al, 2011).
One question that was recently raised is the potential for a “rebound effect” when stopping the use of soft multifocals, as occurs with atropine (Chia et al, 2014). A recent study suggests that this may not occur with multifocal contact lenses, although further research is needed (Cheng et al, 2015). Lasowski and Sheardown (2016) demonstrated the ability to effectively load and release atropine from silicone hydrogel contact lens materials, which opens the door to combination anti-myopia products.
Randomized clinical trials have also shown that orthokeratology may reduce axial elongation by up to about 55% per year (Charm and Cho, 2013; Cho and Cheung, 2012; Hiraoka et al, 2012). As with soft contact lenses, these studies support the idea that children can safely and effectively wear overnight orthokeratology lenses. However, as with any medical device, post-market studies indicate that the rate of complications for both children and adults increases when contact lenses are used outside of controlled trials (Bullimore et al, 2013; Eydelman et al, 2012).
More long-term data show continued myopia control effects with orthokeratology (Hiraoka et al, 2012), but a recent study suggests that there may be a rebound effect after children stop wearing orthokeratology lenses (Swarbrick et al, 2015). Although an interesting preliminary finding, due to the smaller sample size and contralateral-eye design, further research is needed to fully understand the after-effect of stopping orthokeratology (Swarbrick et al, 2015).
Looking Ahead The CooperVision MiSight lens (Figure 1) received CE marking as a method to slow myopia progression, but there is no myopia control contact lens cleared for use in the United States. Orthokeratology also does not have an FDA indication for use as a myopia control device. Thus, the use of either soft multifocals or orthokeratology to slow the progression of myopia is done off-label in the United States and in many other countries.
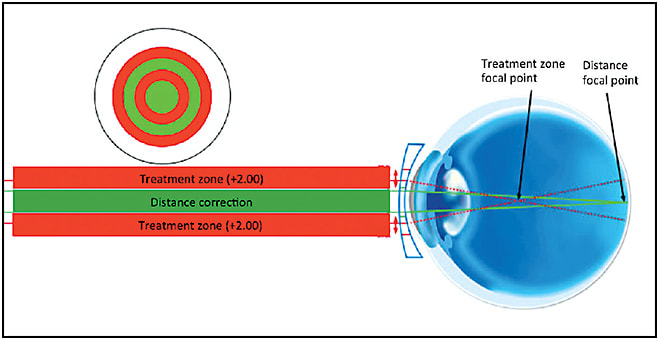
Figure 1. Design and concept of CooperVision’s MiSight lens.
More research is needed to fully understand how to optimize treatments, including what dose and duration of treatment is needed and when treatment may be stopped. However, given our knowledge of the increasing prevalence and visual and ocular health consequences of myopia, there is a clear and growing need for an approved drug or cleared device to offer patients the ability to at least slow the progression of their myopia.
Smart Contact Lens Technologies
Patients can now monitor multiple aspects of their health and wellness minute by minute with the help of “smart technologies.” They can check their heart rate, metabolic activity, sleep habits, and other health data with their smartphone, watch, or other personal devices. As chronic diseases can now be tracked and monitored directly by patients, the hope is that it will lead to improvement in their health (Phan et al, 2015). Advances in smart materials in optics and engineering have also allowed the development of contact lenses that can be used as sensors and actuators in the human body.
Current Development Sensimed offers the Triggerfish, a contact lens that provides continuous measures of IOP (Figure 2) (Hervas Ontiveros et al, 2013). The device is comprised of a silicone-based contact lens with an embedded sensor, and it is designed to measure IOP every five minutes for up to 24 hours. The Triggerfish has already undergone safety and efficacy studies in human clinical trials (Mansouri et al, 2015; Tan et al, 2015; Tojo et al, 2015).
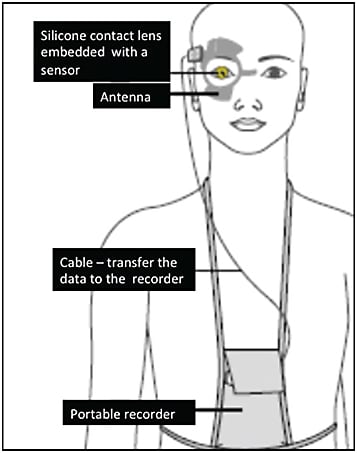
Figure 2. Sensimed’s Triggerfish contact lens sensor for monitoring IOP.
As would be expected, its use was associated with some mild blurred vision, conjunctival hyperemia, and superficial punctate keratitis, but it was generally well tolerated and able to produce repeatable measures of IOP (Mansouri et al, 2012). Another concern raised is the lack of validation with traditional IOP measurements (Phan et al, 2016). The Triggerfish is labeled as a single-use device and currently has CE-mark approval. The FDA also recently cleared the device to be marketed in the United States. Given the known diurnal fluctuations in IOP, the Sensimed Triggerfish could allow practitioners to better understand the state of the disease and effects of glaucoma medications.
Glucose-sensing contact lenses have been under development since the early 2000s (Ascaso and Huerva, 2015). The goal is to provide a non-invasive, continuous measure of glucose levels such that patients could more easily manage their diabetes. Tear glucose levels are up to five times higher in diabetics than in normal patients (Sen and Sarin, 1980); however, the concentration of glucose in tears is still very low, and there is a lag of up to 20 minutes before glucose levels change in the tears (Phan et al, 2016).
To assist with this, Google and Novartis recently announced their plans to develop a glucose-sensing contact lens using a unique embedded three-dimensional electrode sensor (Patel et al, 2011; Teutsch et al, 2014) (Figure 3). The prototype device contains a low-power wireless microchip and antenna that would sync with a mobile device and could record glucose levels as often as every second (King, 2014; Ascaso and Huerva, 2015).

Figure 3. Novartis and Google are developing a glucose sensing contact lens.
Obviously, there are many manufacturing and development challenges to making such a device tolerable to patients, disposable or able to be disinfected, and manufactured at a reasonable cost that would be acceptable to patients. But the potential of being able to offer a method of noninvasively and continuously monitoring glucose levels for the 25 million Americans who suffer from diabetes is no doubt exciting for both eyecare providers and general physicians.
Jiang (2011) and colleagues at the University of Wisconsin-Madison received a National Institutes of Health grant to develop accommodative contact lenses for presbyopia. The researchers incorporated a tunable liquid microlens into a contact lens and aim to provide up to 4.00D of near “accommodation” (change in focus). To power the device, a solar energy circuit will be used to harvest and store energy while the lens is being worn (Jiang, 2016).
Looking (Even Further) Ahead Clearly, many of these big ideas won’t be available in the near future and will likely face a lot of challenges with not only manufacturing, but also regulatory approval, especially in the United States. Google hopes to have a glucose sensing contact lens available on the market by the year 2019-2020 (King, 2014). There’s no clear indication of when other smart contact lenses might be commercially available.
Embracing New Contact Lens Technologies
Imagine a world in which an eyecare practitioner prescribes anti-myopia contact lenses to an 8-year-old child and glucose-sensing contact lenses for her 13-year-old diabetic sibling. For their mother, the practitioner first measures diurnal IOP with a contact lens and then treats her glaucoma with continuous release drug delivery contact lenses.
The possibilities for revolutionizing the way we manage patients’ ocular and systemic health are extraordinary. But, as these new devices enter the market, it is important to consider that there will likely be many challenges to adopting them into general practice. Industry sponsors, regulators, healthcare insurers, practitioners, and patients all have their own risk/benefit concerns and reasons for embracing or rejecting new medical treatments. As practitioners, when a new device hits the market, there are often still some questions regarding their long-term safety and efficacy. Practitioners are well trained to “do no harm” and thus may delay adopting a new treatment until it is well proven.
There should always be a careful balance between employing established treatments and embracing new ones. However, it is ultimately our duty as healthcare providers to stay current with new treatments—i.e., to read and understand the research—such that we keep our profession moving forward and provide our patients with the best evidence-based care possible. CLS
For references, please visit www.clspectrum.com/references and click on document #246.

| Dr. Chao joined Dr. Richdale’s lab as a post-doctoral scholar in 2014 after graduating from the School of Optometry and Vision Science at University of New South Wales. |

| Dr. Richdale is an assistant professor and director of the Clinical Vision Research Center at the SUNY College of Optometry. She is a consultant or advisor to Johnson & Johnson Vision Care Inc. (JJVCI) and Alcon Labs. She has also received a research grant from JJVCI, Alcon, and Shire Pharmaceuticals. |