


TIPS TO GROW YOUR PRACTICE
FOUR STRATEGIES FOR PRACTICE GROWTH
Tips on how to get contact lens patients in the door and keep them there.
DAVID L. KADING, OD, & MILE BRUJIC, OD

We all know the challenges of having a practice. Getting patients in the door has always been a major challenge, and attracting new patients has forever been difficult. Yet, we somehow go to work and look at our schedules day in and day out and see that some patients have elected to choose us as their eyecare providers yet again. Many of these patients need vision correction, and some of them make up our contact lens-wearing patient base.
Around 34% of most practices are made up of contact lens wearers (Figure 1). Most practices see approximately 23 contact lens patients each week, and contact lenses represent around 25% of the total profit for most practices (Nichols, 2015). Well-run practices certainly have a higher percentage and show progressive growth over the years. Contact lens-wearing patients certainly have the potential to be the most profitable in the practice, especially over the life of the patient.
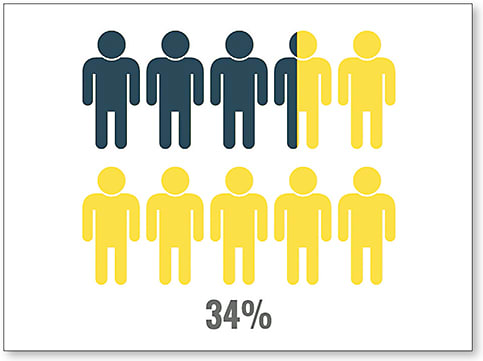
Figure 1. Contact lens wearers in a typical practice.
Consider that many contact lens patients return to the office for contact lenses about every 15 months, while spectacle-only wearers return about every 2.5 years. Therefore, we realize that there is a significant opportunity to help out these patients and to generate more revenue (Goldberg, 2006). One way to do that is to ensure that these patients have both spectacles and contact lenses. This is especially beneficial because nearly 60% of contact lens-wearing patients purchase their eyeglasses from their eyecare provider (McLean, 2006). Because of the additional purchasing of contact lenses and glasses, plus the additional service fees, one estimate calculates a contact lens-wearing patient to be 91% more profitable compared to a spectacle-only patient over a six-year time period (Akerman, 2010) (Figure 2). If this segment is so profitable, shouldn’t we spend more time growing this part of our practice? Here, we look at four key ways to enrich our contact lens practice.
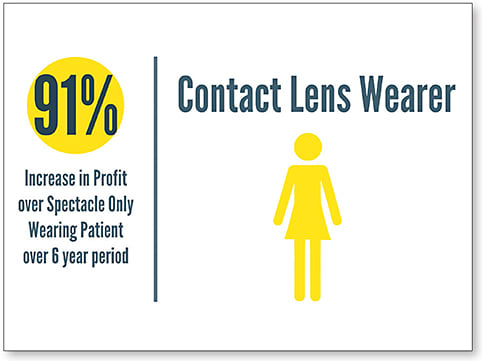
Figure 2. Profitability of spectacle-only patients versus spectacle and contact lens patients.
1. PLUG THE BUCKET
If you want to grow your practice, it is critically important to not only focus on bringing in new business, but also to evaluate which patients are no longer part of the practice or, in our case, are no longer wearing contact lenses. Contact lens dropout remains a major issue. Although we have improved the technologies and the quality of both lenses and solutions over the years, our dropout rates remain very high. Just take these statistics to heart. Of the total contact lens-wearing base, 48% are between the ages of 18 to 34 years, 22.5% are between 35 and 44 years, 16.3% are between 45 and 54 years, and 13.2% are older than 55 years. These numbers indicate that less than 30% of all contact lens wearers are over the age of 45 years (Nichols, 2015) (Figure 3).
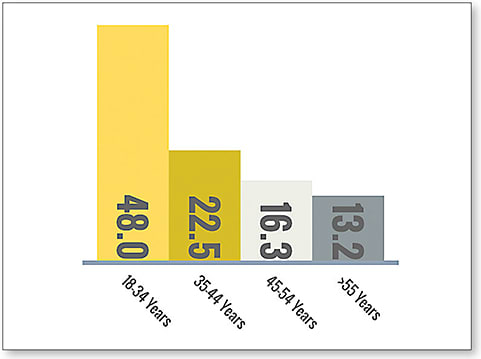
Figure 3. Percentage of patients wearing contact lenses ages 18 to 55+ years.
When we realize that this segment generally is the largest percentage of patients in our offices, it presents an incredible opportunity to work hard to keep these patients in their lenses. Additionally, these patients tend to have a slightly higher disposable income and may elect to choose options when it comes to their eyewear. This means that they may choose to wear contact lenses on a part-time basis and select different spectacle lenses for other times. With regard to their lenses, they may choose daily disposables and wear a distance-only lens for some activities and multifocals for other activities.
Between 50% to 94% of patients who wear contact lenses will report to their practitioner with problems related to their lens wear (Dumbleton et al, 2013), and the problems that they most often present with are discomfort and dryness (Riley et al, 2006). One study that looked at 453 lens wearers found that 24% of them had discontinued lens wear, 76% of them reported dryness, and 67% reported discomfort (Richdale et al, 2007). With statistics like these, is it any wonder that our contact lens patient base seems to have flatlined? It is imperative that we as practitioners discover and solve the problems of our patients.
We have been part of the movement over the years to upgrade our patients’ lenses and care solutions to keep them in the best technology possible. For some patients, this will give them an initial level of comfort that they can appreciate. It may also prolong their comfortable lens-wearing experience by one to two years.
However, we have discovered that the problem is rarely the lens or solution itself. By no means do we hesitate to move our patients to better technology. In fact, our preference is to move patients to daily disposables when available. But this change must be associated with additional measures. We wholeheartedly believe that identifying and treating the underlying cause of the lens discomfort is the best mechanism that we can use to help patients stay comfortable in their lenses. If patients return to the clinic after a year or two of lens wear and note that their eyes feel more dry than they did in the past, we acknowledge that it was not the lenses that changed. Instead, we elect to focus on the ocular surface.
Many patients who have symptoms of dryness reveal signs of dry eye disease. These patients present with some similar signs of dryness as contact lens wearers, and unless we look for them carefully, we may miss them. One such measure on which we place a lot of emphasis is lid wiper epitheliopathy (LWE) (Figure 4). This condition is marked by a disruption to the cells of the lid wiper region. Between 67% to 80% of symptomatic lens wearers have LWE, while only 13% to 32% of asymptomatic patients revealed signs of the condition (Korb et al, 2002; Yeniad et al, 2010). If this high of a percentage of symptomatic patients have this condition, it certainly warrants careful observation when looking at who may drop out of lens wear.
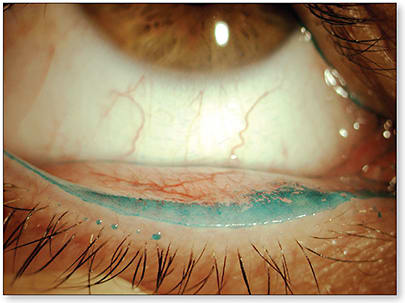
Figure 4. Lower lid with lid wiper epitheliopathy.
Our treatments also focus heavily on the meibomian glands. A study by Lemp and colleagues (2012) showed that 86% of patients who have dry eye have meibomian gland disease as a contributor (Figure 5). Another study showed that lens-wearing patients between the ages of 25 and 40 years had similar meibomian gland atrophy as non-wearing patients who were 60 to 69 years old (Arita et al, 2009). Finally, a study looking at changes to meibomian glands over time for lens-wearing patients revealed that there was a significant decrease in morphology and function that occurs early in contact lens wear but seems to stabilize for the remainder of their lens-wearing years (Alghamdi et al, 2016) (Figure 6). Ergo, we do not take this condition lightly. Instead, we look for any sign that a patient’s meibomian glands are showing a decrease in function. We carefully evaluate the meibomian glands either by applying gentle pressure with our thumb to their eyelid or by using a tool that can consistently apply the force of a standard blink. If we do in fact see a decrease in the oil production, then we will begin more aggressive treatment for our lens wearers than for their spectacle-wearing counterparts because of the related rate of contact lens dropout. Our aim is to improve their end-of-day comfortable wearing time.
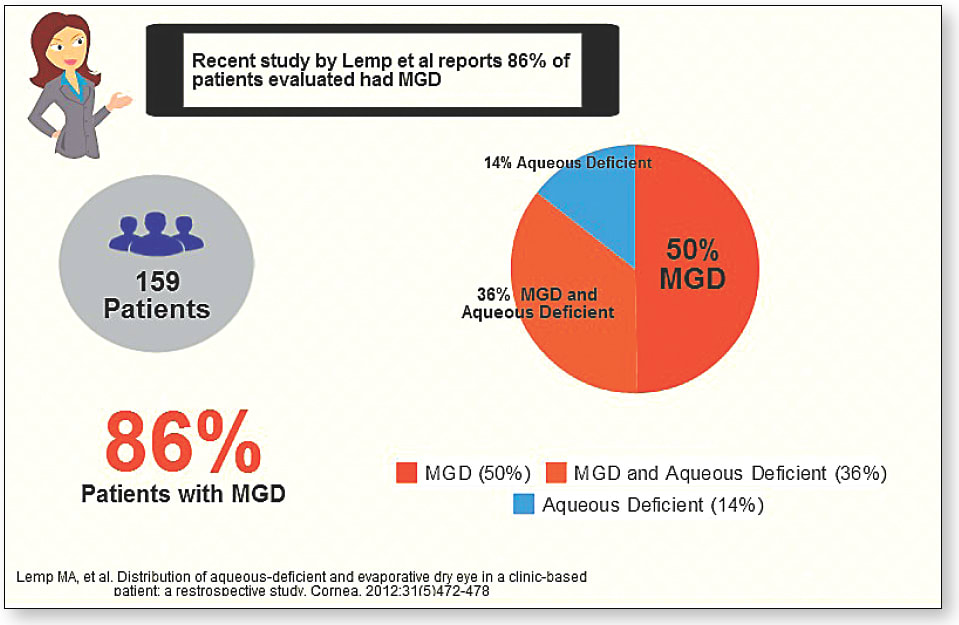
Figure 5. Prevalence of meibomian gland disease.
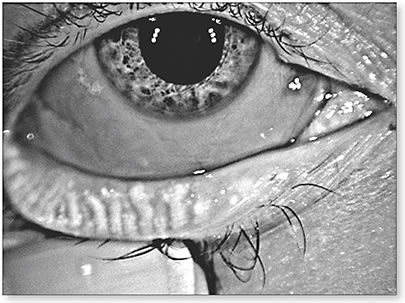
Figure 6. Meibography that shows moderate atrophy in the meibomian glands.
Our treatments for patients who have contact lens-related dryness relate very much to the treatments we use for regular dry eye patients. Depending on clinical signs, we generally start with a high-quality ocular nutrient containing omega-3s and lifitegrast or cyclosporine in an effort to increase the quality and quantity of tears produced. We use other treatments as well, but these are our mainstay.
Plugging the bucket on dropouts helps us to grow our contact lens base perhaps more than any other strategy. It is our first line of defense in passively growing our contact lens-wearing patient base.
2. CONVERSION OF CURRENT PATIENTS
Our current patient base is full of patients who wore contact lenses in the past, but have elected to no longer wear them. Additionally, some of the patients have never even considered wearing contact lenses, usually because of concerns regarding comfort, cost, and/or fear of the unknown. Many of these patients would be delighted to wear contact lenses again, or for the first time, if they knew what their options were.
We feel that the greatest way to convert patients into contact lenses for the first time, or back into contact lenses, is to share with them the benefits of part-time wear. Making a commitment to change your method of vision correction can be daunting, particularly if you have never worn contact lenses or dropped out of wearing them because of discomfort. However, nearly every glasses wearer has times during his or her week during which a contact lens would be beneficial. Whether for cosmetic reasons, sports, or other hobbies, contact lenses provide a patient incredible freedom.
As such, we often present our patients with the option of using daily disposable lenses. When given the option for occasional wear with costs that impact them only on the days on which they are wearing the lenses, patients see contact lenses as another option rather than something that they must use.
Traditionally, we have presented our patients with the option of wearing glasses or contact lenses. For those patients who choose spectacles, we now emphasize that they also have with the freedom to choose whether and when they want to wear contact lenses. This has presented a fantastic entry into lens wear. We did not have this presentation option with contact lenses that had two-week and monthly replacement schedules; patients saw only the cost of everyday wear, cleaning, and commitment as something in which they were not interested.
In addition to the incredible impact that occasional wear can have on a patient, it is also good for your practice. We have found that patients who elect to be refit into contact lenses also elect to continue wearing them year in and year out. Often, a sale of lenses within the office does not yield a year’s supply; with part-time wear, a years’ worth of lenses can last longer than 12 months. However, these patients traditionally buy eyeglasses with the same frequency as they would have had they not also chosen contact lenses. These patients bring the additional benefit to the practice of their contact lens service fees and the sale of any boxes of lenses they may elect to purchase.
We find patients who formerly dropped out of lens wear and are revived to part-time wear to be some of the most grateful and happy patients.
3. INCREASED SEGMENTS
As we have traveled the world speaking about contact lenses with practitioners, we have seen a consistency among practitioners who excel in their contact lens practice. They eagerly treat patients who have astigmatism, presbyopia, keratoconus, post-surgical eyes, progressing myopia, and every other type of patient who may benefit from wearing contact lenses.
Several years ago, we challenged all of the practitioners in our office. For every non-contact lens patient we saw in the clinic, we simply had to state the following: “You are an excellent candidate for contact lenses, have you ever considered them?” This has opened up incredible dialog with patients who have had all sorts of problems. Some patients have told us that their previous practitioner told them that they were not eligible. Others have said, “Well, I wear bifocals so [contact lenses] won’t work.” For others, they had never really considered contact lenses but welcomed the conversation. Although some chose not to move forward at that exam, we had planted a seed in their mind about the possibility of using contact lenses. The next time they are outside without an umbrella or at the beach on vacation, they may reconsider and elect to move forward at their next office visit.
Astigmatism Patients who have cylinder have traditionally been seen by practitioners (and themselves) as a challenge for contact lenses. For this reason, these patients can be the most loyal.
With small amounts of cylinder—and if the patient struggles with rotational stability—using a lens that has multiple base curves or diameters can bring about significant improvement. If a daily disposable or frequent replacement lens is not available for the patient, most are very grateful to be fit into a custom lens (Figure 7).

Figure 7. A patient wearing a custom soft lens.
Within the United States, we have a plethora of fantastic soft lens laboratories that are capable of designing lenses for nearly any patient who has astigmatism. We have found that there has been a shift away from focusing on base curve alone; more and more of the labs are designing lenses based upon corneal diameter and sagittal depth. When the depth of the lens matches that of the cornea, we find that lenses are much more stable.
And, of course, we cannot forget the recent innovations in daily disposable lenses. We have seen the greatest innovation in the advancement and utilization of daily disposable torics in our offices. Our astigmatic contact lens base appears to have risen steadily over the years as more of these patients have elected to wear lenses due to their disposability, ease of use, and convenience.
Presbyopia For the majority of practices, presbyopes comprise the largest segment of patients. But as stated previously, less than 30% of all lens wearers are over the age of 45 years (Nichols, 2015). Although contact lenses do not provide the same vision as spectacles, they do provide aspects of vision that spectacles cannot. In our practice, we have observed that success in presbyopic patients happens when we can adequately communicate the lens’ strengths and drawbacks and then get those lenses onto patients’ eyes so they can observe what we are talking about. While some patients may elect not to move forward with the technology, we see incredible loyalty from the patients who do convert. And, for the patients who do not convert into multifocal lenses, we offer them daily disposable distance lenses for occasional use.
One segment of the population that generally never moves into contact lenses is the emmetropic presbyopes; these patients tend to be the most frustrated with their lack of clear vision. We find that if these patients have strong binocularity, they may not succeed with any contact lens options. However, if a patient’s binocularity is not strongly bound between the two eyes, we will use a multifocal contact lens in front of the nondominant eye. This will typically provide emmetropic presbyopes the opportunity to obtain adequate near vision with minimal disruption to their distance vision.
We will then release them for a week of lens wear, and we will check back with them to modify their vision if necessary. These patients frequently come back very happy with the independence that the multifocal lens provides from reading glasses. And, although the vision at near may not be as good as with reading glasses, they will oftentimes enjoy the freedom that that the lens provides to function without reading glasses.
Keratoconus Keratoconus patients (Figure 8) are the most loyal patients whom we encounter. If a practice is capable of adequately meeting the vision and comfort needs of its keratoconus patients, those patients will remain in the practice indefinitely. We have even had patients who have moved to other states fly back to see us in our specialty contact lens practices.
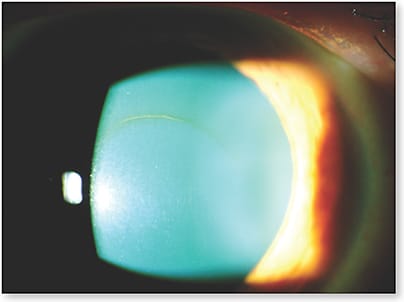
Figure 8. Keratoconus patient with striae and a Fleischer Ring.
To grow our specialty practices, we have done a few things to enhance the growth of our keratoconus patient base. First, we placed a video on our website about our specialty practice and that we specifically focus on keratoconus. Second, we placed advertisements online for patients who are searching for help with their keratoconus. This has brought in many new keratoconus patients over the years. Third, we have reached out to other practitioners in our area and mentioned that we would be honored to help them with this patient base. The gratitude that many practitioners have expressed is remarkable. It certainly is a win-win-win for the patient, our practice, and the other practitioners who no longer want to treat keratoconus patients.
Post-Surgical Patients For many patients who have undergone refractive surgery, the thought of wearing contact lenses again is furthest from their mind. Unless their visual acuity has suffered significantly, they may choose to stay in eyeglasses even if they would have a substantial improvement with contact lenses. We encourage these patients to try lenses to see how their vision can be improved beyond what spectacles can provide.
Orthokeratology Orthokeratology lenses are a great way to correct patient refractive error (Figure 9). In our practices, they are used mostly for myopia control. As most studies have noted, orthokeratology lenses can reduce the progression of myopia by around 50% (Cho et al, 2005). We use this statistic and many practitioners’ clinical experience to our patients’ advantage.
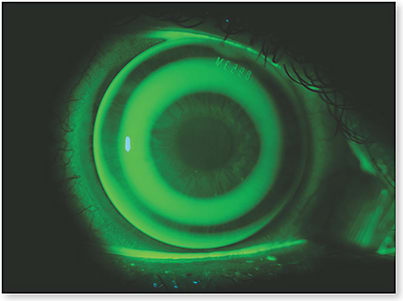
Figure 9. A patient wearing an orthokeratology lens.
By providing orthokeratology, we have been able to expand our custom lens practice into the pediatric segment. We also find that parents talk. After fitting patients, we tell parents that we would be honored to help anyone else they know who is going through progression of refractive error like their child is. This has helped to grow our patient referrals, and it has helped a large host of patients as well.
4. NEW TECHNOLOGIES
As we have enhanced our specialty in lenses over the years, we have looked for new ways to expand our patient base. As such, we look to new technologies to help improve what we currently do. Over the last 10 years, the industry has seen incredible advancements. For example, scleral lenses are being utilized at an increasing rate.
While we were among the few fitting sclerals in 2004, they are now a mainstay (Figure 10). Orthokeratology has also risen to new heights. We have newer and improved lens materials with advanced surface capabilities. Labs are coming out with new designs to enhance the optics that they lathe into them. We have an array of soft keratoconus lenses. And, soft lens companies have worked tirelessly to make daily disposables available in a spectrum of corrections for astigmatism, presbyopia, and high sphere as well as for patients experiencing dryness.

Figure 10. A patient wearing a scleral lens.
Embracing new technology in our offices allows us to expand to patient types that we have not yet considered. In addition, we can bring patients back into the office who have failed in the past or are struggling with their current contact lenses.
REFOCUS
When we look at our practice as an opportunity for better patient care, we will naturally strive to provide that care to more patients. This helps bring about better patient care and also plugs the hole of patients dropping out of lens wear. With these strategies, we feel that your practice will grow and your impact will bring improvement to the quality of life of your patients. CLS
For references, please visit www.clspectrum.com/references and click on document #252.
Dr. Brujic is a partner of Premier Vision Group, a three-location optometric practice in northwest Ohio. He has received honoraria in the past two years for speaking, writing, participating in an advisory capacity, or research from Alcon Laboratories, B+L, Bruder, Optovue, RPS, SpecialEyes, and VMax Vision and has received research funding from Optovue and SpecialEyes.
Dr. Kading owns the Specialty Dry Eye and Contact Lens Center in Seattle. He is the co-owner of Optometric Insights with Dr. Mile Brujic. He has received honoraria for consulting, performing research, speaking, and/or writing from Alcon Laboratories, Allergan, Bausch + Lomb, CooperVision, Johnson & Johnson Vision Care, Oculus, OptoVue, RPS Detectors, Paragon Vision Sciences, TearScience, Valeant Pharmaceuticals, Valley Contax, VSP, ZeaVision, and Zeiss. Follow him on Twitter @davekading.