




Prior to the introduction of modern scleral lenses, we were somewhat cavalier to the presence of pingueculae in our contact lens wearers. The corneal lens designs were often far enough away from the lesions that they created little or no problems with contact lens wear. Our soft contact lenses often “vaulted over the top” or draped over the pingueculae and also caused only minor problems unless the pingueculae were excessively elevated.
However, this all changed when we discovered the benefits of scleral lenses for our patients who cannot be managed with corneal GP or soft lenses. We now have become aware of the significant number of our patients who have clinical or subclinical pingueculae.
Techniques for Managing Scleral Elevations
In recent years, the industry has discovered a number of creative ways to limit the interaction of scleral lenses with a wide range of elevated conjunctival lesions, such as pingueculae, pterygia, and filtering blebs.
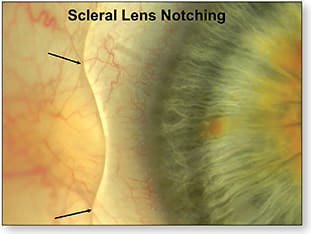
Lens Notching One such technique is often referred to as “notching.” With this technique, the laboratory removes a portion of the scleral lens periphery, resulting in a “notch” that positions around the elevated lesion (Figure 1). The lens can be properly orientated by placing toricity onto the posterior surface of the lens (a 150-micron height differential between the two principle meridians). Once the lens has orientated, a permanent marker can be used to identify the position and area over which the notch is to be placed.
Lens Periphery Modifications Another technique is the use of a quadrant-specific lens periphery or a microvault in the lens periphery. A microvault creates a flute at the edge of the scleral lens to vault over any conjunctival elevations.
Lens Diameter Modifications Yet another technique is to simply modify the scleral lens diameter. Figure 2 shows a 16.5mm diagnostic lens on a patient who has advanced keratoconus. It is easy to see that the lens edge is resting over the top of the patient’s pinguecula.

We then placed a diagnostic lens that had an overall diameter of 14.8mm on this patient. Figure 3 shows how the smaller lens diameter positioned just inside of the lesion.

Clinical experience has taught us that smaller-diameter scleral contact lenses (i.e., 14.8mm) can achieve many of the fitting principles of larger-diameter scleral lenses; however, this is only possible for patients whose corneal diameter is smaller than normal—such as 11.5mm or less. We have learned that it is often difficult to achieve appropriate limbal clearance when smaller-diameter scleral lenses are used for corneal diameters that are in the normal range or are larger than normal. CLS