


Iron Staining in Corneal Ectasia: Keratoconus Versus Pellucid Marginal Degeneration

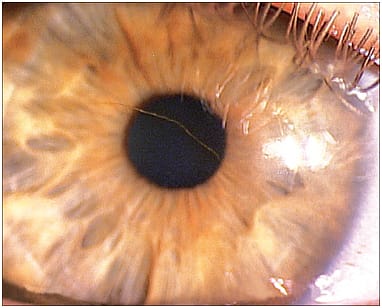
This 32-year-old male presented with severely reduced vision in his right eye. Subsequent evaluation, including corneal topography, led to an initial diagnosis of asymmetric keratoconus versus pellucid marginal degeneration (PMD). The visual axis in the left eye was minimally involved, and the cornea was clear. Passing through the visual axis of his right eye (pictured) is linear iron staining of the cornea.
Iron and the Eye
Iron is essential to human metabolism; for example, the iron in hemoglobin molecules binds to oxygen.1 Dietary iron is absorbed through the small intestine and is lost in sweat, exfoliated skin, intestinal cells, and menstruation. Because the body cannot actively secrete iron, excess iron is stored in some tissues, including corneal tissues. Superfluous iron levels can lead to the formation of oxygen free radicals and resulting toxicity. Several studies suggest that iron may be involved in the pathogenesis of cataract and age-related macular degeneration.1
Iron deposits of the cornea are located in the basal epithelial cells and are often visible upon slit lamp examination.1 It is often not possible to visualize subclinical corneal iron staining using white light slit lamp examination. Every and colleagues demonstrated the value of using ultraviolet photography to identify corneal ferritin staining that could not be visualized using white light.2
Corneal iron lines occur in the normal aging cornea (Hudson-Stähli line), in keratoconus (Fleischer ring), at the base of pterygia (Stocker’s line), and adjacent to filtering blebs (Ferry’s line).1 Extracellular iron, which is normally present in the tear film, is bound to lactoferrin secreted by the lacrimal glands. The literature regarding iron lines associated with keratoconus is abundant, but iron staining is infrequent in PMD.3
Keratoconus or PMD?
Keratoconus and PMD are the most common forms of corneal ectasia. It is not certain whether PMD and keratoconus are dissimilar diseases or whether they are distinctive clinical presentations of the same underlying disease process. Although the “crab claw” configuration seen in the topography of the right eye (Figure 2) is very common in PMD, it is not necessarily diagnostic. This topographic feature is also seen less frequently in keratoconus. Fleischer rings are often seen in keratoconus, but may be subclinical (i.e., not visible under white light biomicroscopy).

In this case, the late onset (early 30s) suggests PMD; typical onset in keratoconus is in the teens. The configuration of the topography and the significant asymmetry between the eyes (Figure 2) also suggests PMD.3
Both keratoconus and PMD are considered to be non-inflammatory disorders. Hungarian researchers compared the levels of 11 inflammatory markers in the tears of patients who had keratoconus (55 eyes) and PMD (nine eyes). With one exception, there were no statistical differences; matrix metalloproteinase-9 (MMP-9) tear levels were significantly higher in the PMD patients.4
In conclusion, keratoconus and PMD are forms of corneal ectasia that share many common characteristics, but in some cases may be difficult to differentiate. In this patient, we achieved very good vision and comfort with hybrid lenses.
References:
- Loh A, Hadziahmetovic M, Dunaief JL. Iron homeostasis and eye disease. Biochim Biophys Acta. 2009 Jul;1790:637-649.
- Every SG, Leader JP, Molteno AC. Ultraviolet photography of the in vivo human cornea unmasks the Hudson-Stähli line and physiologic vortex patterns. Invest Ophthalmol Vis Sci. 2005 Oct;46:3616-3622.
- Maharana PK, Dubey A, Jhanji V, Sharma N, Das S, Vajpayee RB. Management of advanced corneal ectasias. Br J Ophthalmol. 2016 Jan;100:34-40.
- Pásztor D, Kolozsvári BL, Csutak A, Berta A, Hassan Z, Ujhelyi B, Gogolák P, Fodor M. Tear Mediators in Corneal Ectatic Disorders. PLoS One. 2016 Apr 13;11:e0153186.