




A 10-year-old female was recently referred to our clinic to evaluate her complaint of dry eye, which is atypical for such a young child. She had a previous diagnosis of allergic conjunctivitis and severe, chronic, anterior blepharitis that was only mildly responsive to treatment. She also had an excavated, moderate-sized corneal scar OS, inferior to the visual axis with associated pannus and neovascularization. This was secondary to a previous bacterial corneal ulcer; however, she had never worn contact lenses.
Biomicroscopy revealed grade 2 flaking with mild-to-moderate posterior lid margin redness on all lids, while vital dyes highlighted a reduced tear breakup time and grade 3 to 4 superficial punctate keratitis OD and OS. The palpebral conjunctiva showed a moderate papillary reaction with grade 1 diffuse injection, consistent with her prior diagnosis of allergic conjunctivitis.
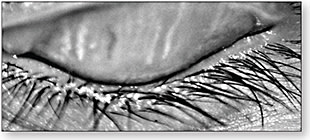
Meibography showed almost 100% complete dropout of all meibomian glands in the lower lids (Figure 1), and only five to six partially-atrophied glands remained in each upper lid (Figure 2).

Ocular Rosacea in Children
Rosacea often goes unrecognized in children, as the telltale dermatological signs are frequently absent. Kids who have ocular rosacea generally have chronic blepharitis and conjunctival hyperemia, punctate epitheliopathy, corneal pannus/neovascularization, and meibomian gland disease that doesn’t respond particularly well to topical therapy. Progression to corneal ulceration and/or scarring is common (Cetinkaya and Akova, 2006). Clinicians should be suspicious when children present with dry eye complaints and/or ocular surface disease, even if there are no dermatologic findings (Donaldson et al, 2007).
Treatment
Our patient was treated in-office with lid margin exfoliation, which removed all flakes and scales. She was started on home maintenance therapy that consisted of daily warm compresses with a commercial mask followed by lid scrubs and q.i.d. instillation of a lipid-based artificial tear. We also prescribed 750mg of a flavored oral liquid omega-3, along with erythromycin ointment q.h.s., a mast-cell stabilizer/antihistamine q.d., and a short course of topical corticosteroids. Daily, 0.05% topical cyclosporine ophthalmic emulsion was also prescribed for long-term anti-inflammatory therapy. Although not U.S. Food and Drug Administration approved for children under 16, ophthalmic cyclosporine is a safe and effective option for the treatment of severe pediatric ocular surface conditions (Ozcan et al, 2007; Keklikci et al, 2008). It can help to manage chronic meibomian gland inflammation by reducing dysfunction and improving tear film stability (Prabhasawat et al, 2012). Advanced treatments for MGD were unaffordable at this time.
This regimen has stabilized the patient for the past six months; however, therapy with systemic erythromycin or doxycycline may be necessary in the future. Both are beneficial in older children who have ocular rosacea (Cetinkaya and Akova, 2006; Donaldson et al, 2007; Nazir et al, 2004). CLS
For references, please visit www.clspectrum.com/references and click on document #258.