




Scleral lens fitters are increasingly using more sophisticated designs to successfully fit a wide variety of indications. A key design element is the haptic back surface. Spherical, toric, or multi-meridian designs can be manufactured depending on patients’ scleral geometry.
Spherical Versus Toric Back-Surface Haptics
Optical coherence tomography and corneo-scleral topography have shown that the scleral shape is non-rotationally symmetrical (van der Worp, 2010; Ritzmann et al, 2015). Additionally, scleral asymmetry is not related to corneal toricity (Kinoshita et al, 2016; Seibert and Jedlicka, 2017). Multiple manufacturers now offer toric fitting sets, and practitioners seem to be prescribing back-surface toricity with increased frequency. The Visser group has shown that patients often prefer haptic back-surface toricity (Visser et al, 2006; Visser et al, 2007).
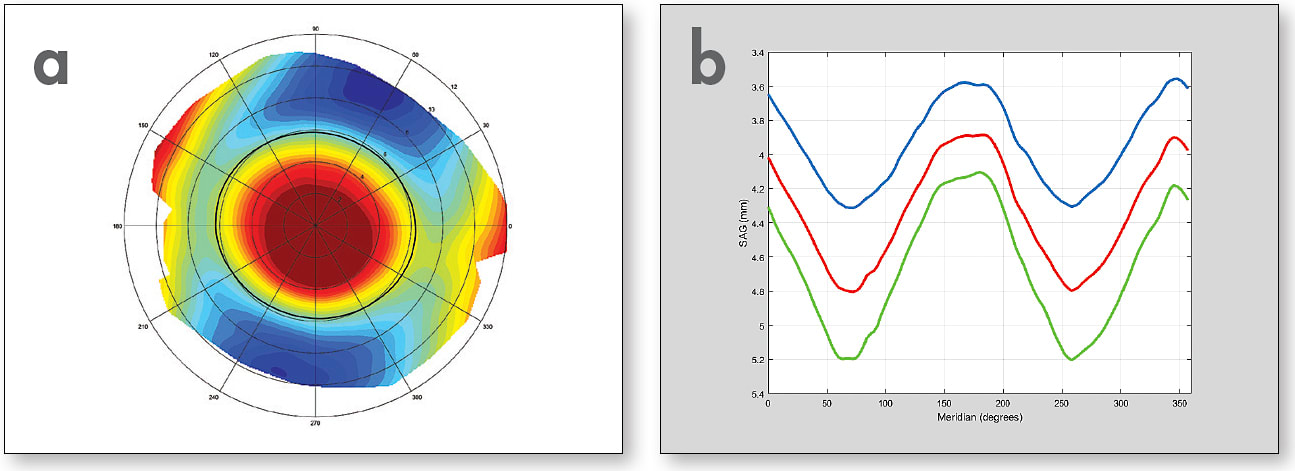
In my practice, scleral lenses that I design have dramatically shifted toward back-surface toricity since I started utilizing corneo-scleral topography (Figure 1 a and b). For a six-month period in 2014 without corneo-scleral topography, 93% of my scleral fits had a spherical back surface, whereas 7% had a toric back surface. In contrast, for a six-month period in 2016 when fitting from corneo-scleral topography, 32% of my fits had a spherical back surface versus 68% with a toric back surface. It is important to keep in mind that some scleras have a relatively spherical shape and will be best fit with a spherical haptic back surface. Fitting these patients with a toric back-surface haptic not only will not improve the fit, but could create a fitting complication.
Toric Versus Multi-Meridian Back-Surface Haptics
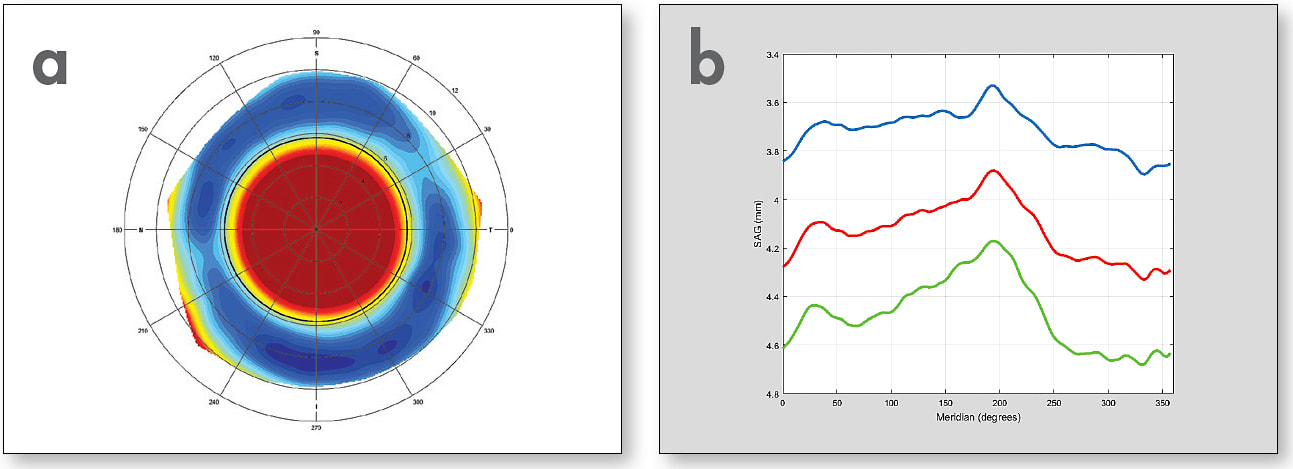
Some patients have scleras with an asymmetric shape that is not definitively toric (Figure 2 a and b). For these patients, a multi-meridian approach is best. They will be best fit using back-surface haptics with four or more primary meridians, not necessarily equidistant, that are tailored for their scleral geometry.
Conclusion
The future of scleral lens design is utilizing spherical, toric, or multi-meridian designs to best fit each individual eye. CLS
For references, please visit www.clspectrum.com/references and click on document #258.