Satisfaction with vision performance involves much more than visual acuity alone.
Contact Lens Spectrum April 1, 2018Vol 33, Issue April 2018Page(s): 38-42, 51
During our long days, most of us challenge our visual system with complex and changing situations such as:
Prolonged near work
High color/contrast resolution demand during digital device use for 10 hours a day or more
Artificial light at work or contrast demands in low-light conditions
Exposure to air-conditioning and heating in the office and when driving
Glare while driving and from approaching vehicles when driving at night
Demands for motion detection and peripheral vision during sports
We take for granted our ability to perform this large and varied array of tasks seamlessly and efficiently. So, any visual disturbance arising over the course of the day immediately raises our awareness and potentially lowers our vision satisfaction. Attempts to determine the quality of visual perception with a measure of satisfaction are confounded by cognitive factors, linguistics, attention, adaptation, and environment. Visual satisfaction is also influenced by factors such as contrast sensitivity, stereoacuity, and visual fields as well as by visual acuity.1 And visual discomfort contributes significantly to visual satisfaction, as seen with long-term digital device use, 3D displays, and virtual reality systems.2,3
Vision satisfaction also fluctuates throughout the day and with different tasks. Blurred vision, vergence difficulties, and accommodative problems are common complaints after prolonged near work; these are mostly related to visual environmental factors, primarily glare, lighting, screen resolution, and workstation arrangement.4,5,6
We hypothesize that vision satisfaction is driven primarily by three dimensions of vision: spatial awareness, discriminating efficiency, and visual endurance. The first two dimensions relate to functional vision and describe our ability to execute the visual tasks that our visual system evolved to perform: near, intermediate, and distance tasks and color, contrast, and movement detection. The third dimension—visual endurance—provides a measure of the transient impact of biological and environmental factors on vision satisfaction.
SPATIAL AWARENESS
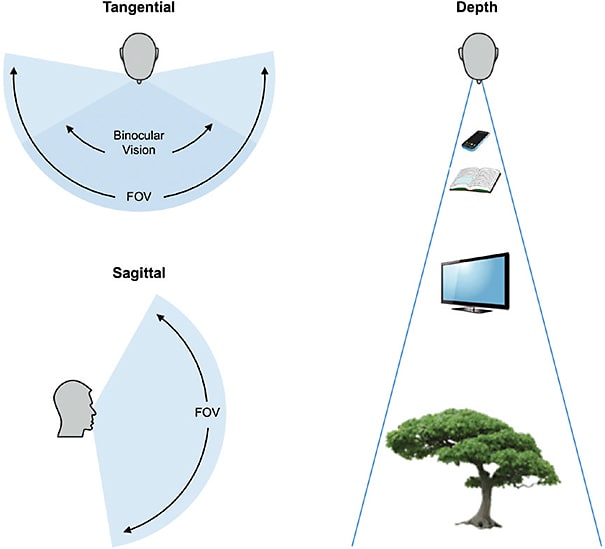
Broadly, spatial awareness refers to the perception of objects in the surrounding environment, understanding their meaning and location as well as a projection of their status in the near future.7 While much of this process is cognitive, it is underpinned by two critical elements of the visual system: visual field and depth perception (Figure 1).
Figure 1. Spatial awareness depends on two critical elements of the visual system: visual field and depth perception.
In a human eye, field of view (FOV) varies with facial anatomy, giving an asymmetric FOV of approximately 60° nasally, 60° superiorly, 70° inferiorly, and 100° temporally.8 As a result, a typical binocular FOV is 135° sagittal and 200° tangential.9
Depth perception refers to the ability to assess the distance of objects within the environment. This is largely a monocular phenomenon, driven by cues that include motion parallax,10 optical expansion,11 perspective, texture, and blur.12
DISCRIMINATING EFFICIENCY
Discrimination refers to the recognition of differences between elements in the environment. Discriminating efficiency is defined as the ratio of correct discriminations to the total number of discriminations. While much of this process is cognitive, it is underpinned by four critical capabilities of the visual system: resolution, chromatic contrast sensitivity, motion detection threshold, and stereoacuity (Figure 2). Resolution refers to the minimum distance at which two points can be distinguished. It is often specified as the minimum angle of resolution in units of arc seconds.13 Chromatic contrast refers to differences in chromaticity in a scene or image.14 It contributes significantly to the perception of contour and object recognition in natural scenes.15 Motion detection threshold refers to the minimum displacement needed for accurate assessment of direction of motion.16 Stereoacuity is the smallest depth interval that a subject can detect; it is specified by the threshold difference in binocular disparity in arc seconds.17
Figure 2. Contributions of the visual system to discriminating efficiency include: (A) resolution, (B) chromatic contrast, (C) motion detection, and (D) stereoacuity.
VISUAL ENDURANCE
Patients expect the same seamless, comfortable vision at any point in time, any day, regardless of the task or environment. Specifically, they expect a lack of awareness of their spatial and discriminating vision efficiency. However, evolution has given humans an innate capacity to notice changes and to ignore constant, stable stimuli.
Consequently, any biological or environmental factor triggering a change in vision quality immediately raises awareness and is registered as, at best, inconvenience or, at worst, discomfort. In fact, research has recently demonstrated an association between quality of vision and ocular surface sensation.18
Environmental factors affecting vision involve tasks to which our visual system has not had time to evolve, such as prolonged near work, night driving, or digital device use. Prolonged near tasks and digital devices present a unique set of issues that also include ocular dryness due to reduced blinking. Night driving issues vary from noticing lane demarcations or reading street signs to the glare from oncoming headlights.
Environmental factors affecting vision relate to dryness-inducing air conditioning or heating, whether in a car, office, or store; low humidity as during air travel; and sudden changes in luminance, such as moving from indoors to outdoors or photostress due to glare from the sun. Diabetes and dry eye are among biological sources of vision fluctuation.19,20 The tear film, another key refractive element in the visual system, can also introduce transient refractive effects when unstable.21,22
Hence visual endurance, the third dimension of visual satisfaction, provides a measure for the expectation of seamless vision across tasks and over time. To summarize, visual satisfaction is driven by much more than visual acuity alone and encompasses visual endurance as well as many aspects of functional vision (Figure 3).
Figure 3. Summary of factors involved in visual satisfaction.
MEETING PATIENT NEEDS
Now that we have a better understanding of visual satisfaction, how can we ensure that the vision correction that we prescribe meets our patients’ needs? While we cannot do much more currently in the areas of spatial awareness and discriminating efficiency, it is in the area of visual endurance that we can likely make an impact. Let’s use what we know about patient satisfaction with contact lenses to explore this concept further.
It is widely accepted clinically that soft contact lenses provide excellent vision to patients. Recently, we carried out a prospective, randomized, subject-masked, three-arm parallel-group clinical study. Eligible subjects were non-presbyopic, habitual wearers of spherical silicone hydrogel contact lenses within the power range available and had uneventful systemic and ocular histories. They gave informed consent to the study, which had ethics committee approval. The subjects were randomly selected to wear one of three study lenses on both eyes on a daily wear basis, with follow-up visits occurring at one and two weeks after the initial dispensing. A total of 240 subjects completed the study as the total cohort. Figure 4 plots Snellen visual acuity in contact lens wearers during a two-week wear period. More than 93% of wearers achieved 20/20 or better visual acuity post-fit, at one week, and at two weeks.
Figure 4. Snellen visual acuity in a study of contact lens wearers over a two-week period.
But the story is quite different when we ask patients about their level of satisfaction with aspects of visual performance using the Contact Lens User Experience (CLUE) Questionnaire.23 CLUE scores are statistically designed such that average lens performance has an aggregate CLUE score of 60. Data mining was used to analyze the CLUE Vision satisfaction responses of more than 6,000 pre-presbyopic patients aged 18 to 39 years old who were wearing a variety of different spherical contact lens brands from several manufacturers across a range of lens powers.
On a scale of 0 (low satisfaction) to 120 (high satisfaction), this population scored in the low 60s, indicating slightly above-average satisfaction but hardly a resounding clinical outcome. Response variance shows a small percentage of patients seemingly satisfied with their vision, but also a large proportion of patients scoring their habitual vision below 50; this indicates that the soft contact lens industry is not meeting the expectations of a significant proportion of this population. Investigating further, they were more likely to dislike their vision at the end of the day and to experience fluctuation in their quality of vision.
Another recent study examined a day in the life of soft contact lens wearers.24 Subjects agreed to respond every two hours to text messages probing their activities, environments, symptoms, emotions/moods, comfort, satisfaction, and vision quality. Subjects were aged 18 to 39 years, wore contact lenses at least four days per week and at least 12 hours per day, and had visited their eyecare professional within the past two years. Their habitual lenses were spherical and from any brand from any manufacturer. A total of 243 subjects completed the study; 142 of the subjects were reusable lens wearers, and 101 were daily disposable wearers.
A majority (62%) experienced a decline in comfort, overall lens satisfaction, and vision quality over the course of the day (Figure 5). Those in that “decline” group often had busier lifestyles and experienced at least 10 different activities throughout the day, particularly tasks that involved reading, using a device with a screen, and doing housework. Among symptoms reported, decliners were most likely to complain of tired eyes (69%) and dry eyes (65%).
Figure 5. Comfort, lens satisfaction, and vision quality responses over one complete day.24
So, although patients may record excellent vision when measured by Snellen acuity, probing more deeply into aspects of visual performance reveals that many are less than satisfied with their current lenses.
CONCLUSIONS
Vision satisfaction is influenced by three dimensions: spatial awareness, discriminating efficiency, and visual endurance. Visual acuity alone does not provide a full picture because vision satisfaction relates to functional vision as well as to changing tasks and environments that are challenging our visual system more than ever. As we have seen, current contact lens products are not fully satisfying patients’ visual needs, particularly as they go through their busy days and experience many different activities.
It is in the area of visual endurance that clinicians currently have the potential to make the biggest impact on patients’ visual satisfaction. Current best practices would be to ensure that a contact lens accurately corrects the refractive error, including any astigmatism; that the fit is stable; and that the optical quality of the lens is optimal. It is very important that the material can support a stable tear film over the course of a long day.
Currently, vision and comfort are the principal measures that we use to assess the performance of a contact lens, and Snellen visual acuity is the usual method of assessing vision. In the future, we may need to consider a wider range of vision metrics, assess visual symptoms in greater depth, and find new ways of monitoring performance across the course of a day’s wear if we are to truly satisfy our patients.
There is also an opportunity for further product innovation to enhance visual performance and drive greater levels of patient-reported visual satisfaction. We look to the future where these needs are fulfilled through advanced designs that may be more adapted or specialized for particular applications. CLS
KEY INSIGHTS
Our visual system is challenged by multiple tasks and situations over the course of the day.
Vision satisfaction can fluctuate throughout the day and with different tasks.
Vision satisfaction is driven by spatial awareness, discriminating efficiency, and visual endurance.
Many soft contact lens wearers report fluctuating and declining overall satisfaction during the day.
Snellen visual acuity alone may not be a good indicator of vision satisfaction in contact lens wear.
New metrics and in-depth assessment are needed to elicit vision satisfaction in contact lens wear.
Successful future soft contact lens products should address the unmet need for visual endurance over the course of the day.
REFERENCES
El-Gasim M, Munoz B, West SK, Scott AW. Associations between self-rated vision score, vision tests, and self-reported visual function in the Salisbury Eye Evaluation Study. Invest Ophthalmol Vis Sci. 2013 Sep 27;54:6439-6445.
Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic Physiol Opti. 2011 Sep;31:502-515.
Kooi FL, Toet A. Visual comfort of binocular and 3D displays. Displays. 2004 Aug;25:99-108.
Birnbaum MH. Optometric Management of Near Point Disorders. Boston: Butterworth-Heinemann. 1992 Dec 23. pp 121-160.
Sheedy JE, Parsons SD. The visual display terminal eye clinic: clinical report. Optom Vis Sci. 1990 Aug;67:622-626.
Sheedy JE. Vision problems at video display terminals: a survey of optometrists. J Am Optom Assoc. 1992 Oct;63:687-692.
Endsley MR. Theoretical underpinnings of situation awareness. In: Endsley MR, Garland DJ, eds. Situation Awareness Analysis and Measurement. Mahwah, NJ: Lawrence Erlbaum Associates, 2000. pp 1-21.
Savino PJ, Danesh-Meyer HV, eds. Color Atlas and Synopsis of Clinical Ophthalmology—Wills Eye Institute—Neuro-ophthalmology. Lippincott Williams & Wilkins, 2012 Sep 19.
Schneck ME, Dagnelie G. Prosthetic vision assessment. In: Dagnelie G, ed. Visual Prosthetics: Physiology, Bioengineering, Rehabilitation. Springer Science & Business Media, Boston. 2011 Mar 3. pp 385-412.
Swanston MT, Gogel WC. Perceived size and motion in depth from optical expansion. Percept Psychophys. 1986 May;39:309-326.
Schwartz S. Visual Perception: A Clinical Orientation. McGraw Hill Education. 2009 Dec 11.
Jenkins FA, White HE. Fundamentals of Optics. McGraw-Hill Book College, 1976 June 1.
Luo MR, ed. Encyclopedia of Color Science and Technology. Springer, 2016 June 2.
Hansen T, Gegenfurtner KR. Color contributes to object-contour perception in natural scenes. J Vis. 2017 Mar 1;17:14.
Turano K, Wang X. Motion thresholds in retinitis pigmentosa. Invest Ophthalmol Vis Sci. 1992 Jul;33:2411-2422.
Howard IP, Rogers BJ. Perceiving in Depth. Volume 2: Stereoscopic Vision. Oxford University Press. 2012 Feb 24.
Rao SBS, Simpson TL. Impact of blur on supra-threshold scaling of ocular discomfort. Invest Ophthalmol Vis Sci. 2015 Apr;56:2304-2311.
Koffler M, Raskin P, Geyer O, Yust I. Blurred vision: an overlooked initial presenting symptom of insulin-dependent diabetes mellitus. Isr J Med Sci. 1990 Jul;26:393-394.
Koh S. Mechanisms of visual disturbance in dry eye. Cornea. 2016 Nov;35 Supp1:S83-S88.
Montés-Micó R, Alió JL, Muñoz G, Pérez-Santonja JJ, Charman WN. Postblink changes in total and corneal ocular aberrations. Ophthalmology. 2004 Apr;111:758-767.
Koh S, Maeda N, Hirohara Y, et al. Serial measurements of higher-order aberrations after blinking in normal subjects. Invest Ophthalmol Vis Sci. 2006 Aug;47:3318-3324.
Wirth RJ, Edwards MC, Henderson M, Henderson T, Olivares G, Houts CR. Development of the Contact Lens User Experience: CLUE Scales. Optom Vis Sci. 2016 Aug;93:801-808.
Mathews K, Daigle B, Alford J, Jedraszczak AM. Exploring variability in soft contact lens performance. Poster presented at the American Academy of Optometry Annual Meeting. 2015 Oct.
Philippe Jubin is Senior Manager Lens Design at Johnson & Johnson Vision Care, Inc., where he leads the Lens Design and Clinical Metrology teams.
Dr. Buch is Senior Principal Research Optometrist at Johnson & Johnson Vision Care, Inc.
Dr. Nankivil, BSAE, MSBME, PhD, is Staff Engineer Vision Products at Johnson & Johnson Vision Care, Inc. He works to relate visual perception and optical stimuli and to develop novel contact lenses.