



A 13-year-old male recently presented to our clinic with an interest in soft contact lenses. He is a student and plays soccer on his junior varsity team. His spectacle Rx was right eye –6.50 –0.50 x 180 and left eye –6.50 –0.50 x 180. Central simulated K readings were similar in both eyes—43.00 (7.85) @ 180 and 44.00 (7.65) @ 90—and his horizontal visible iris diameters (HVIDs) were 11.8mm in both eyes.
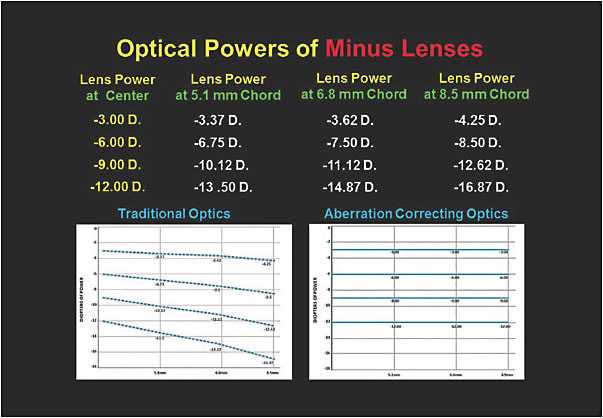
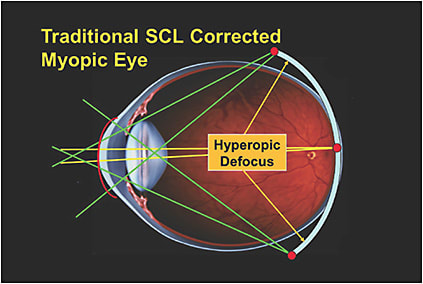
Now…this looks like a pretty straightforward case to prescribe one of our many daily disposable soft contact lenses; but, let’s take a closer look at this from a slightly different perspective. This 13-year-old is already a moderate myope. If we correct this adolescent’s foveal refractive error with a soft lens of –6.25D, he will most likely see a clear 20/20. However, we must keep in mind that the minus lens power in his daily disposable soft lenses will increase from the geometric center of the lens to the periphery. Figure 1 shows how a –6.00D soft contact lens will have a dioptric power of –6.00D in the center and –7.50D at a chord of 6.8mm. This increase in the mid-peripheral minus power brings the rays of light to focus posterior to the retina, resulting in a hyperopic defocus (Figure 2). Today, we know that hyperopic defocus is a rather strong stimulus for the eye to further increase its axial elongation. A closer look at Figure 1 shows that the amount of induced hyperopic defocus increases as the myopic lens power increases.
Look Beyond Refractive Error
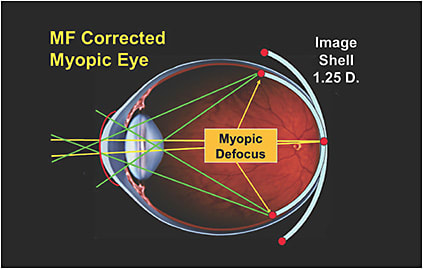
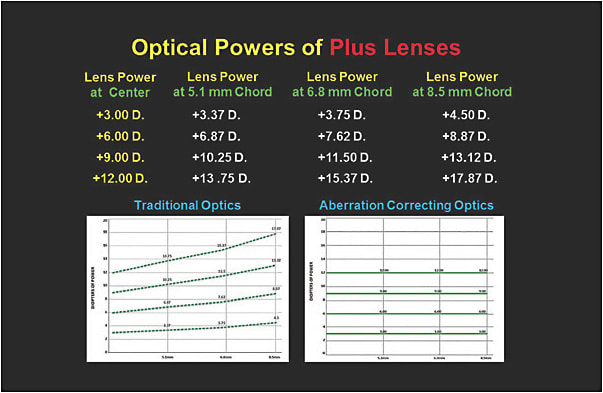
Therefore, the question now is, what soft contact lens might be best for this 13-year-old? From an optical perspective, we would suggest a center-distance multifocal soft contact lens with a central correction of –6.25D and a peripheral add power of approximately +1.50D. This lens design will simultaneously correct both the individual’s foveal and peripheral refractive errors, resulting in a more desirable myopic defocus (Figure 3). Figure 4 illustrates the optical changes of plus-powered lenses from the geometric center of the lens to the periphery.
This case illustrates how modern myopia research has influenced our prescribing of soft lenses in younger patients who have progressive myopia. Therefore, what started out as a clear case for traditional daily disposables (that increase in minus power from center to periphery) dramatically changed to a multifocal soft lens design that incorporates some myopia-controlling optics. CLS