



There are an estimated 140 million contact lens wearers worldwide,1 with 40.9 million residing in the United States.2 More than 90% of these individuals wear soft contact lenses. Hydrophilic soft lenses were invented by Otto Wichterle in the 1960s,3 with the first commercially available soft lens being introduced in the United States in 1971. GP materials, specifically silicone acrylate, were first introduced in 1974. Prior to that, “hard contact lenses” were manufactured out of polymethyl methacrylate (PMMA). Shortly after the introduction of soft lenses to the marketplace, reports of adverse events such as vascularization, corneal edema, giant papillary conjunctivitis, and corneal inflammation and infection began to surface.4 Nearly 50 years after the advent of soft contact lens (SCL) and GP materials, many of these same complications that were noted early on continue to be commonly diagnosed.
A recent editorial by Professor Nathan Efron states that contact lens wear is “intrinsically inflammatory,” so there is little question that if something inherently triggers an inflammatory response (to some degree), then undesired effects will ensue.5 Each structure of the eye is subject to these uninvited events, including the eyelids, the palpebral conjunctiva, the bulbar conjunctiva, the tears, and the cornea. These insults, both by SCLs and GPs, are proposed to occur through one—or a combination—of four basic mechanisms. The four proposed mechanisms are hypoxia, mechanical irritation, toxicity, or microbial contamination (Table 1).
| MECHANISM | GP LENS | SOFT LENS | OCULAR STRUCTURE(S) INVOLVED |
|---|---|---|---|
| HYPOXIA | |||
| Vascularization | Yes† | Yes | Cornea – Epithelium/Stroma |
| Microcysts | Yes | Yes | Cornea – Epithelium |
| Bullae | Yes | Yes | Cornea – Epithelium |
| Vacuoles | Yes | Yes | Cornea – Epithelium |
| Blebs | Yes | Yes | Cornea – Epithelium |
| Polymegethism | Yes | Yes | Cornea – Epithelium |
| MECHANICAL | |||
| Meibomian Gland Atrophy | Maybe | Yes | Eyelid |
| Lid Wiper Epitheliopathy | Yes | Yes | Palpebral Conjunctiva |
| Lid Parallel Conjunctival Folds | Yes | Yes | Bulbar Conjunctiva |
| Mucin Balls | No | Yes | Tear Film |
| Superior Epithelial Arcuate Lesions | No | Yes | Cornea – Epithelium |
| 3 o’clock and 9 o’clock Staining | Yes | Yes | Cornea – Epithelium |
| Vascularized Limbal Keratitis | Yes | No | Limbus |
| CLPC‡ | Yes | Yes | Tarsal Plate |
| Limbal Stem Cell Deficiency* | Yes | Yes† | Cornea – Epithelium |
| TOXICITY | |||
| Solution-Induced Corneal Staining | Yes† | Yes | Cornea – Epithelium |
| Incomplete Neutralization – Peroxide | Possible | Possible | Cornea – Epithelium |
| MICROBIAL CONTAMINATION | |||
| Aseptic Corneal Infiltrative Events | Yes | Yes | Epithelium, Anterior Stroma |
| Infectious Corneal Infiltrative Events | Yes | Yes | Potentially All Corneal Layers |
| †Condition is more common with soft contact lenses. ‡CLPC is thought to have both mechanical and lens deposit (allergy-related) mechanisms. *Stem cell deficiency may be multifactorial including hypoxia, toxicity, and mechanical etiologies. |
|||
HYPOXIA
Hypoxia during contact lens wear has been extensively studied and was a significant issue, particularly when PMMA lenses were in use. Under non-contact lens-wearing conditions, the cornea—which is an avascular tissue—obtains the majority of its oxygen from the atmosphere. If a material provides insufficient oxygen to the cornea (or the post-lens tear film becomes thick, as it can in scleral lens wear), then metabolic changes inevitably occur. These metabolic changes can affect the corneal endothelium, stroma, epithelium, and the limbus.
Starting with the epithelium, evidence of hypoxic distress may manifest as microcysts,6 vacuoles,7 bullae,7 thinning of the epithelium,8 and decreased efficacy of ocular surface defense mechanisms. Microcysts are intra-epithelial cystic formations that likely consist of broken down cellular debris. These cysts exhibit reversed illumination and are generally identified in patients who wear lower-oxygen-transmissible (lower-Dk/t) lenses. Unless an extreme amount is present, microcysts are typically asymptomatic and do not affect vision. If it is determined that there is an abundance of microcysts, then switch to a higher-Dk/t lens. In addition, if the lenses are being worn on an extended wear basis, they should be discontinued.
Corneal epithelial vacuoles—which are similar in size to microcysts but exhibit a non-reversed illumination characteristic—typically accompany corneal hypoxia and epithelial edema.9 Epithelial bullae tend to be more oval, clustered, generally greater than 40µm, and have indistinct margins.10 The etiology of bullae is unclear at this time and may be related to hypoxia or to mechanical compression. This compression is thought to weaken epithelial tight junctions, which may allow excess fluid to accumulate in the extracellular space, resulting in the bullae.
Corneal vascularization generally develops from a hypoxic post-lens environment or from chronic ocular surface inflammation. This oxygen-deficient environment leads to a release of pro-angiogenic cytokines from metabolically stressed cells that, in turn, leads to the development of blood vessels in the formerly avascular corneal tissue.11 Vascularization has been estimated to be present in 1% to 34% of the contact lens-wearing population, with a lower frequency in GP wearers; this is presumably due to greater tear exchange associated with GP lenses. The primary risk factors are wearing lenses overnight, high refractive errors, and low-oxygen-permeable (low-Dk) materials. Contact lenses that provide an oxygen transmissibility of 30 to 40 Fatt units or greater are thought to prevent the development of vascularization.11 Practitioners do need to consider that the central Dk/t of a lens is often misrepresentative of the Dk/t at the edge of the optic zone and the lenticular (if present). Therefore, with regard to high refractive errors, material selection is important.
Clinical signs of corneal hypoxia secondary to contact lens wear are no more evident than with the corneal endothelium. These changes can be transient, as with endothelial blebs,12 or permanent, such as polymegethism. With endothelial blebs and polymegethism, the prevailing etiology is thought to be an increase in corneal acidity due to low-Dk/t lenses. This increase in acidity is due to a lack of oxygen, resulting in an increase in lactic acid, and an increase in carbon dioxide, leading to excess carbonic acid (hypercapnia).12 In the case of blebs, the affected endothelial cell(s) transiently swell, resulting in a relative dark focal spot when performing specular reflection. The bleb formation quickly peaks, then nearly returns to normal while the lens is on. Once the lens is removed, the blebs disappear. Fortunately, endothelial blebs are thought to be of minimal concern.12
Polymegethism is thought to be a long-term corneal response due to an acidic environment.13 With polymegethism, the typical cellular distribution is affected, which manifests as hexagonal cells of various sizes. Though the shape of the cell is altered, the cellular function is presumed to be minimally affected. With modern materials that offer high-oxygen-transmissibility, polymegethism will likely be less severe, if present at all.
Hypoxia has also been associated with epithelial thinning,8 and hypoxic conditions in the presence of a contact lens have been shown to increase Pseudomonas binding.14
Although many of the complications listed above are no longer observed on a daily basis due to an increased use of silicone hydrogel and hyper-Dk GP contact lens materials, they remain a threat if the corneal metabolism is altered.
Hypoxia has also recently been a readily discussed topic with regard to scleral lenses.15 This type of GP lens is gaining in popularity and, generally, will have a center thickness of 350 to 400 microns with a tear reservoir that varies from patient-to-patient or can even vary dramatically across a patient’s own ocular surface. If a lower-Dk lens material is selected or the tear reservoir is excessively thick, a patient may be susceptible to the hypoxic corneal changes listed above.
MECHANICAL IRRITATION
Meibomian Gland Atrophy Arita et al found meibomian gland atrophy secondary to contact lens wear.16 When comparing the meibomian gland integrity of age-matched CL wearers against non-CL wearers, the CL wearers demonstrated more gland atrophy. This gland atrophy may be due to desquamated epithelial cell accumulation near the gland orifice or, more likely, through chronic irritation from CL wear. This chronic irritation is irrespective of material, with GP and SCL materials demonstrating equivalent gland loss. Although no direct correlation has scientifically been determined linking CL discomfort to meibomian gland atrophy, it is clear that CL wear affects the gland architecture; this very likely will be associated with ocular surface dryness.
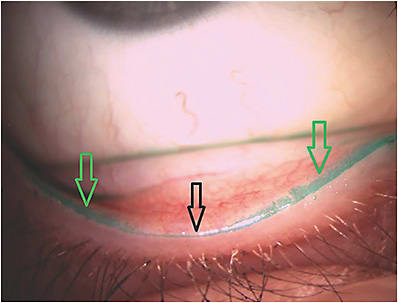
Lid Wiper Epitheliopathy and Lid-Parallel Conjunctival Folds Dry eye is a common issue related to contact lenses, but it will not be discussed in this article as this topic has been discussed extensively in Contact Lens Spectrum (July 2018). Two dry eye-related complications that will be discussed are lid wiper epitheliopathy (LWE) (Figure 1) and lid-parallel conjunctival folds (LIPCOFs). LWE was first discussed by Korb and colleagues in 2002.17 This condition is essentially due to mechanical friction between the lid wiper portion of the inferior and superior lid palpebral conjunctiva and the anterior surface of the contact lens. If there is insufficient lubrication between these two surfaces, the lid epithelium will be exposed to shear-like forces resulting in epitheliopathy. The LWE will stain with fluorescein, but it is much easier to discern with lissamine green or rose bengal (note: the latter is much more irritating to patients). To manage this condition, advise patients to temporarily discontinue lens wear, and recommend artificial tears to encourage tissue healing. With recurrent LWE, consider refitting the patient into a contact lens with a lower coefficient of friction, and recommend consistent artificial tear use.
LIPCOFs may not be a complication of contact lens wear, but rather a reliable sign of ocular surface dryness, which, of course, can be exacerbated by contact lens wear. Via slit lamp biomicroscopy, LIPCOFs appear as small conjunctival folds that run parallel to the lid and are located just temporal and nasal to the inferior limbus. The presence of LIPCOFs has been recently identified as a strong predictor of dry eye.18 Practitioners should evaluate their patients for this sign and, if present, should address the dry ocular surface to improve the likelihood of successful contact lens wear.
Mucin Balls These spherical entities range from 20µm to 200µm in size and consist of ocular surface mucins. The mucin balls are considered to be caused by a mechanical shearing effect between the lens and the cornea, and they get lodged into the epithelium. Mucin balls are most readily identified with silicone hydrogel lenses, but they can be observed with hydrogel lenses as well. Overnight wear tends to be associated with the greatest amount of mucin ball formation, as it is hypothesized that a lack of tear exchange results in a mucin-rich environment. Mucin balls are benign and become easily dislodged upon lens removal.
There is conflicting literature about the presence of mucin balls and the risk of corneal inflammatory events (CIEs). A 2010 study19 suggested that the presence of mucin balls may be protective, while a more recent article from 2017 suggests the reverse.20 If present on a patient’s eye, it would be prudent for the practitioner to discuss contact lens practices that minimize CIE risk.
Superior Epithelial Arcuate Lesions Moving posteriorly to the tear layer, the epithelium can be mechanically altered by contact lens wear in a variety of ways. One mechanical corneal epithelial alteration is a superior epithelial arcuate lesion (SEAL), which is an arcuate band of epithelial staining located superiorly that is approximately 1mm to 2mm wide by several millimeters in length. Most of the time, SEALs are asymptomatic; therefore, they are typically only identified during a routine examination.
The prevailing mechanism is thought to be a high-modulus contact lens along with a tight upper lid.21 The excessive lid pressure creates a shearing effect that disrupts the epithelial surface. Management is relatively straightforward. Lens wear should be discontinued for several days to a week, and artificial tear use can be considered. The patient should then be fit into a lower-modulus lens, preferably with a slightly larger diameter to distribute the bearing of the lens over a larger surface area.
Nasal and Temporal Epithelial Disruption A condition that is unique to GP lens wear is nasal and temporal corneal epithelial disruption, often referred to as 3 o’clock and 9 o’clock staining. This staining pattern results from inadequate tear distribution over the nasal and temporal peripheral cornea. The insufficient tear distribution may result from a laterally displaced lens,22 an incomplete blink, or excessive edge clearance. If you envision excessive edge clearance, the eyelid drapes over the edge of the contact lens, bridges over the peripheral corneal region, and then re-opposes the ocular surface. Due to the bridging effect, the tear film over that portion of the cornea is not readily replenished, resulting in epithelial desiccation. Management of this condition can include changing to a soft lens (if appropriate) or to a larger-diameter corneal or scleral lens, redesigning the peripheral curves of the corneal GP, and encouraging more thorough blinks.
Vascularized Limbal Keratitis (VLK) Unique to GP lenses, VLK generally develops in the nasal and temporal limbal region, very similar to 3 o’clock and 9 o’clock staining. While the tissue affected by VLK likely has overlying epithelial staining, there is a noted elevation of either the corneal tissue, the conjunctival tissue, or both.23 It is thought that a focally tight nasal or temporal edge may be responsible for initiating VLK. Patient symptoms range from asymptomatic to moderate discomfort and photophobia. Short-term management includes addressing the ocular surface with lubricants and, in some cases, corticosteroids. Long-term management includes reducing wear time, improving the peripheral fit of the lens, attempting a piggyback fit, or use of a scleral lens.
Contact Lens Papillary Conjunctivitis (CLPC) The two current hypotheses for CLPC etiology are mechanical and surface deposits. A patient who has CLPC will typically complain of excessive contact lens awareness in addition to reporting frequent massaging of the eyelid to reposition the lens. Upon slit lamp examination, if the CLPC is relatively localized, a mechanical etiology is suspected.24 If the CLPC is more diffusely spread across the tarsal plate, then an allergic etiology is suspected.24 When CLPC is detected, a temporary discontinuation of lens wear is essential. Following this period of non-lens wear, which may have also included the therapeutic use of a corticosteroid, lens wear can generally be re-initiated but preferably with a daily disposable (DD) modality. A DD lens will minimize deposit issues, which often allows patients to return to successful lens wear and reduces the risk of future CLPC development.
Limbal Stem Cell Deficiency (LSCD) An often overlooked complication of contact lens wear is LSCD. It is estimated that 2.4% to 5% of contact lens wearers will develop a clinical sign of LSCD.25 The pathogenesis of LSCD is multifactorial, including toxicity, hypoxia, lack of lubrication, and mechanical trauma.25 Contact lens-related LSCD generally occurs superiorly and, therefore, the superior lid is thought to be involved. The lid can create a relative hypoxic environment and will also put additional force on the limbal region, inducing increased friction.
This chronic microtrauma alters the limbal stem cells, which allows conjunctival cells or inappropriately differentiated goblet cells to migrate onto the cornea.26 If LSCD is identified, it is prudent to assess the extent. If the condition is significant, then complete discontinuation of lens wear is necessary. If relatively mild, decreasing lens wear, minimizing hypoxia, eliminating care solutions, and using more lubricous materials would be an appropriate course of action.
TOXICITY
Corneal toxicity is generally considered to be chemical damage to the epithelial cells. Many chemicals and some medications can cause epithelial toxicity; for this discussion, chemical preservatives will be the primary topic. A classic example of a topical agent that is associated with toxicity is benzalkonium chloride (BAK), which damages cell membranes.27 When a cell is exposed to a concentration of BAK that it cannot tolerate, it then will lyse, resulting in a characteristic epithelial staining defect. Chemical multipurpose disinfecting solutions (MPDSs) use large molecules, such as polyaminopropyl biguanide or polyquaternium, to serve as microbial disinfectants. These high-molecular-weight chemicals do not tend to predispose patients to a corneal toxicity reaction as compared to BAK.
Although modern preservatives are associated with less toxicity risk, evidence of corneal staining associated with various contact lens care products and contact lens materials has been investigated and reported on numerous times over the last 15 years.28 Simply recommending a change in care solution or lens material/modality will eliminate the problem.
Likewise, a patient may arrive with instant or quick-developing ocular irritation following the application of a lens to the eye when using a hydrogen peroxide-based solution. Although rare, this typically occurs with incomplete neutralization of hydrogen peroxide solutions. Updating the storage case neutralization disk and ensuring appropriate neutralization times, along with patient education, usually solves this problem.
MICROBIAL CONTAMINATION
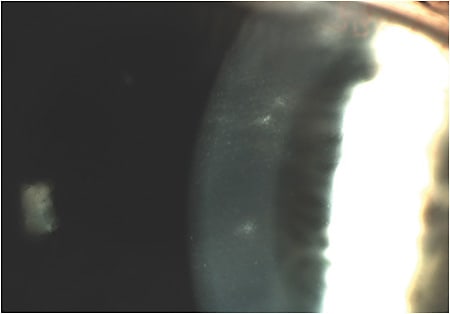
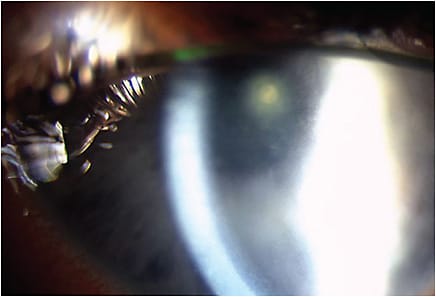
Microbial contamination of contact lenses or contact lens paraphernalia is suggested to be the impetus for the development of CIEs (Figure 2) and the most severe contact lens complications, namely microbial keratitis (MK).29 Microbial contamination of contact lenses and contact lens materials exists in the form of bacteria, fungi, and protozoa, with an increase in severity in that order. Fortunately, frank infectious events (Figure 3) are relatively rare; contact lens bacterial keratitis affects approximately four per 10,000 wearers (overnight wear is ~20 per 10,000),30 fungal keratitis is ~1 per 50,000 wearers,31 and Acanthamoeba keratitis is approximately 1 to 2 per million wearers in the United States.32 Much more common are sterile, or aseptic, CIEs. Symptomatic CIEs are estimated to affect 2% to 4% of wearers and, if asymptomatic events are included, possibly up to 20% of wearers.33 It is somewhat of a misnomer to classify sterile CIEs as sterile, as the presence of non-commensal or an overload of commensal bacteria (or their byproducts) are likely responsible for eliciting the inflammatory response. While CIEs could certainly develop from excessive chemical, mechanical, or metabolic stress—all of which would result in an abundant release of chemotactic factors—most are likely due to microbial contamination.
Possible sources of microbial contamination come from the normal ocular flora, while other sources come from lens wear and care factors that increase the risk of an adverse event. There is a fair amount of overlap with regard to the risk factors for CIEs or MK.33,34 Some risk factors, such as age, sex, immune system genetics, previous CIE, and degree of refractive error are considered non-modifiable, meaning that the individual either always, or for a period of time, carries this inherent risk. Modifiable risk factors, such as smoking, overnight wear, not replacing the storage case, purchase location, silicone hydrogel material, multipurpose solutions, lack of handwashing, and non-DD lens wear are under the volition of the individual and/or practitioner recommendation. These factors, with the exception of purchase location, all increase the likelihood of significant contact lens bacterial bioburden. Exposing lenses, the storage case, or the CL-wearing eye to water increases the risk of contamination, not only with Acanthamoeba, but also with waterborne gram-negative bacteria such as Pseudomonas, Serratia, Achromobacter, Stenotrophomonas, and others.35
There is a significant amount of information on CIEs and MK, including risk factors, diagnostic criteria, and proper management, both of which have recently undergone thorough review.33,34 It is imperative, particularly for MK, to properly differentiate these conditions and initiate effective management immediately. Although CIEs and MK may not often be encountered in an office, practitioners should routinely provide proper patient education and recommend products and wear schedules that minimize the risk of these serious adverse events.
IN CONCLUSION
It should be noted that this particular article features relatively common contact lens complications, but it does not serve as an exhaustive review of all possible contact lens adverse events. CLS
REFERENCES
- Subbaraman LH. In Focus with Current Contact Lens Materials and Designs. Contact Lens Spectrum. 2017 May;32:22-25, 37, 55.
- Cope JR, Collier SA, Rao MM, et al. Contact Lens Wearer Demographics and Risk Behaviors for Contact Lens-Related Eye Infections--United States, 2014. MMWR Morb Mortal Wkly Rep. 2015 Aug 21;64:865-870.
- Wichterle O, Lim D. Hydrophilic Gels for Biological Use. Nature. 1960 Jan 9;185:117-118.
- Binder PS. Complications associated with extended wear of soft contact lenses. Ophthalmology. 1979 Jun;86:1093-1101.
- Efron N. Contact lens wear is intrinsically inflammatory. Clin Exp Optom. 2017 Jan;100:3-19.
- Holden BA, Sweeney DF. The significance of the microcyst response: a review. Optom Vis Sci. 1991 Sep;68:703-707.
- Josephson JE, Zantos S, Caffery B, Herman JP. Differentiation of corneal complications observed in contact lens wearers. J Am Optom Assoc. 1988 Sep;59:679-685.
- Pérez JG, Méijome JM, Jalbert I, Sweeney DF, Erickson P. Corneal epithelial thinning profile induced by long-term wear of hydrogel lenses. Cornea. 2003 May;22:304-307.
- Jones LW, Jones DA. Non-inflammatory corneal complications of contact lens wear. Cont Lens Anterior Eye. 2001;24(2):73-79.
- Nixon AD, Barr JT, VanNasdale DA. Corneal epithelial bullae after short-term wear of small diameter scleral lenses. Cont Lens Anterior Eye. 2017 Apr;40:116-126.
- Yeung KK, Yang HJ, Nguyen AL, Weissman BA. Critical Contact Lens Oxygen Transmissibility and Tear Lens Oxygen Tension to Preclude Corneal Neovascularization. Eye Contact Lens. 2018 Sep;44 Suppl 1:S291-S295.
- Holden BA, Williams L, Zantos SG. The etiology of transient endothelial changes in the human cornea. Invest Ophthalmol Vis Sci. 1985 Oct;26:1354-1359.
- Holden BA, Vannas A, Nilsson K, et al. Epithelial and endothelial effects from the extended wear of contact lenses. Curr Eye Res. 1985 Jun;4:739-742.
- Cavanaugh KJ Jr., Margulies SS. Measurement of stretch-induced loss of alveolar epithelial barrier integrity with a novel in vitro method. Am J Physiol Cell Physiol. 2002 Dec;283:C1801-C1808.
- Michaud L, van der Worp E, Brazeau D, Warde R, Giasson CJ. Predicting estimates of oxygen transmissibility for scleral lenses. Cont Lens Anterior Eye. 2012 Dec;35:266-271.
- Arita R, Itoh K, Inoue K, Kuchiba A, Yamaguchi T, Amano S. Contact lens wear is associated with decrease of meibomian glands. Ophthalmology. 2009 Mar;116:379-384.
- Korb DR, Greiner JV, Herman JP, et al. Lid-wiper epitheliopathy and dry-eye symptoms in contact lens wearers. CLAO J. 2002 Oct;28:211-216.
- Pult H, Bandlitz S. Lid-Parallel Conjunctival Folds and Their Ability to Predict Dry Eye. Eye Contact Lens. 2018 Nov;44 Suppl 2:S113-S119.
- Szczotka-Flynn L, Benetz BA, Lass J, et al. The association between mucin balls and corneal infiltrative events during extended contact lens wear. Cornea. 2011 May;30:535-542.
- Szczotka-Flynn LB, Jiang Y, Stiegemeier MJ, et al; Mucin Ball Study Group. Mucin Balls Influence Corneal Infiltrative Events. Optom Vis Sci. 2017 Apr;94:448-457.
- Holden BA, Stephenson A, Stretton S, et al. Superior epithelial arcuate lesions with soft contact lens wear. Optom Vis Sci. 2001 Jan;78:9-12.
- Preston RW. Understanding 3 and 9 O’clock Staining. Contact Lens Spectrum. 1998 Oct;13:57.
- Grohe RM, Lebow KA. Vascularized limbal keratitis. Int Contact Lens Clin. 1989 Jul-Aug;16:197-209.
- Skotnitsky CC, Naduvilath TJ, Sweeney DF, Sankaridurg PR. Two presentations of contact lens-induced papillary conjunctivitis (CLPC) in hydrogel lens wear: local and general. Optom Vis Sci. 2006 Jan;83:27-36.
- Rossen J, Amram A, Milani B, et al. Contact Lens-induced Limbal Stem Cell Deficiency. Ocul Surf. 2016 Oct;14:419-434.
- Pajoohesh-Ganji A, Pal-Ghosh S, Tadvalkar G, Stepp MA. Corneal goblet cells and their niche: implications for corneal stem cell deficiency. Stem Cells. 2012 Sep;30:2032-2043.
- Dart J. Corneal toxicity: the epithelium and stroma in iatrogenic and factitious disease. Eye (Lond). 2003 Nov;17:886-892.
- Woods J, Jones LW. Pilot Study to Determine the Effect of Lens and Eye Rinsing on Solution-Induced Corneal Staining (SICS). Optom Vis Sci. 2016 Oct;93:1218-1227.
- Szczotka-Flynn LB, Pearlman E, Ghannoum M. Microbial contamination of contact lenses, lens care solutions, and their accessories: a literature review. Eye Contact Lens. 2010 Mar;36:116-129.
- Stapleton F, Keay L, Edwards K, et al. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology. 2008 Oct;115:1655-1662.
- Konda N, Motukupally SR, Garg P, Sharma S, Ali MH, Willcox MD. Microbial analyses of contact lens-associated microbial keratitis. Optom Vis Sci. 2014 Jan;91:47-53.
- Centers for Disease Control and Prevention. Acanthamoeba keratitis fact sheet for healthcare professionals. Available at https://www.cdc.gov/parasites/acanthamoeba/health_professionals/acanthamoeba_keratitis_hcp.html . Accessed on Sept. 24, 2018.
- Steele KR, Szczotka-Flynn L. Epidemiology of contact lens-induced infiltrates: an updated review. Clin Exp Optom. 2017 Sep;100:473-481.
- Carnt N, Samarawickrama C, White A, Stapleton F. The diagnosis and management of contact lens-related microbial keratitis. Clin Exp Optom. 2017 Sep;100:482-493.
- Wang JL, Chen ML, Lin YE, Chang SC, Chen YC. Association between contaminated faucets and colonization or infection by nonfermenting gram-negative bacteria in intensive care units in Taiwan. J Clin Microbiol. 2009 Oct;47:3226-3230.