Many personal and environmental factors contribute to the way that humans see the world.
Contact Lens Spectrum December 1, 2018Vol 33, Issue December 2018Page(s): 32-34, 36-38
Our total visual experience is complex and multifactorial. High-contrast Snellen visual acuity provides information about just one small element of the total visual experience. Although it is the most commonly quantified metric in a clinical setting, visual acuity actually bears little resemblance to the dynamic range of real-world tasks that the visual system encounters.1 To more fully describe an individual’s overall level of visual satisfaction, factors such as spatial awareness, discriminating efficiency, and visual endurance should be considered.2 Additionally, and especially for contact lens (CL) wearers, it must also be recognized that the total visual comfort experience is the sum of both visual and physical sensations.3 This article reviews key measures of visual performance, how they contribute to overall satisfaction in real-world situations, and whether that experience can be influenced by the design of corrective lenses.
KEY MEASURES OF VISUAL PERFORMANCE
Visual Acuity Although easy to measure, visual acuity is a static measure of vision, typically conducted with a high-contrast target under high-luminance conditions. The real world is, of course, much more dynamic; the eye is expected to focus on targets that have a wide variety of spatial frequencies and that are under continually changing conditions of luminance and contrast.
Additionally, a number of factors can influence overall visual performance. These include the quality of the tear film, variation of higher-order aberrations with pupil size, and the role that the brain has in processing aspects of a scene. Given these variables, it is no surprise that we have all probably had the experience of two patients who have similar visual acuity reporting very different overall satisfaction with their vision.
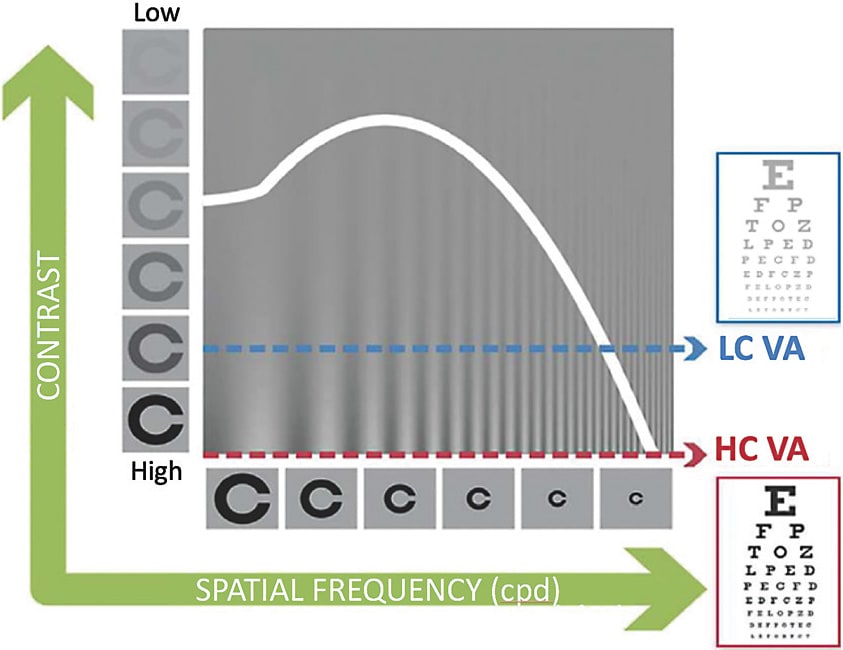
Contrast Sensitivity Function The contrast sensitivity function (CSF) can help describe the quality of vision beyond visual acuity. CSF is measured by presenting a subject with visual targets that vary in both their contrast and their spatial frequency. The threshold of detection is noted for each stimulus. These data allow the CSF to be drawn,4 with the area under the resulting curve said to describe the total visual “space” that can be perceived.5 Better spatial vision is represented by a larger area under the CSF curve. The limitations of visual acuity in describing visual performance are demonstrated in Figure 1, in which this value represents only one extreme point of the CSF. Thus, CSF is thought to be more closely related to daily functional vision.6-8 Differences in visual acuity and CSF are demonstrable in many conditions, including cataract and age-related macular degeneration, in which a significant loss in CSF occurs before acuity is markedly reduced.5
Figure 1. Contrast sensitivity function.
In a research setting, CSF testing requires experienced technicians and is repetitive and time-consuming. However, recent advancements in CSF testing have significantly reduced the duration of the procedure. A computerized approach accelerates estimation of the CSF by leveraging information acquired during the experiment with a priori knowledge about the CSF’s general functional form. Through estimation of CSF parameters, the outcome from a single spatial frequency can help inform estimates across all frequencies.9 Traditional methods for CSF determination can take 30 to 60 minutes. The methodology of the quick CSF (qCSF) produces results in just 10 minutes or less that compare well with those established via traditional testing.9
Because the CSF is thought to be closely related to everyday functional vision,6-8 by quantifying visual performance over a range of spatial frequencies, the CSF—or more specifically, the area under the CSF curve—is very sensitive to changes in visual performance.10 For example, the area under the CSF curve decreases by 0.31, 0.48, and 0.57 log units for people in their 60s, 70s, and 80s, respectively.11
Furthermore, the large increase in acuity that occurs following cataract surgery corresponded to an increase of 0.53 log units on average in five patients.12 In their study to evaluate the performance of the qCSF method to detect changes in visual performance, Hou et al summarize that the literature suggests that 0.15, 0.30, and 0.45 log unit changes of area under the log CSF correspond to mild, medium, and large CSF changes in clinical populations, respectively.10
It is believed that enhancements in formulation, design, and manufacturing process to improve lens performance have demonstrated high subjective visual satisfaction levels in previous clinical studies. Therefore, in addition to assessing and monitoring ocular pathology, the qCSF method has also been used to assess differences in performance of contact lenses. There was a recent randomized, controlled, single-masked, crossover, non-dispensing clinical trial that included 35 individuals who were randomly allocated senofilcon A lenses with design and manufacturing enhancements (test), the test lens with +0.25D spectacle lens in trial frames (positive control), and senofilcon A contact lenses without design enhancement (negative control).13 Outcomes included high-illumination, low-contrast visual acuity; low-luminance, high-contrast visual acuity; and CSF measures. The test lenses resulted in about one-half of a line of improvement in measures of visual acuity compared to the positive and negative control lenses. Likewise, the test lens showed an increase in the CSF of between 14% to 30% compared to the positive and negative control lenses, demonstrating the impact of a design improvement on visual performance.
THE VISUAL SYSTEM
The visual system is complex and includes several variables that can influence total visual experience. We’ve already mentioned neural processing applied by the brain, which can interpolate gaps in a scene based on prior knowledge. In the eye itself, beyond accurate correction of spherical and astigmatic error, higher-order aberrations also contribute to visual quality. Higher-order aberrations such as coma, spherical aberration, and trefoil vary in magnitude based on pupil size, which, in turn, is variable based on illumination level, accommodation, age, and refraction. The quality of the tear film—as the first interface of the optical system with air—is also very relevant, with additional attention required for CL wearers because of the known destabilizing effects of a CL on the tear film.14
Further considerations concern the scatter of light through the visual system. Glare and halos are caused by intraocular forward light scatter. In general, light scattering is the process by which light deviates from its trajectory due to interaction with local irregularities within the ocular media. Intraocular scatter, which is not related to refractive state, may significantly degrade retinal image contrast, particularly when observing scenes that include bright light sources or reflections.15 Similar to the detrimental effects on visual performance of some ocular pathologies, the effects of intraocular scatter are not always well quantified by visual acuity alone, suggesting that other metrics are needed.16
KEY INSIGHTS
Visual acuity only describes one very small part of the total visual experience.
The contrast sensitivity function better describes visual performance, with significant losses found in some ocular pathologies earlier compared to changes to visual acuity.
Measures of visual performance that may be affected by light filtering include disability glare, discomfort glare (squint response), photostress recovery time, chromatic contrast, and visual range.
Real-world situations in which light filtering can make a demonstrable difference include discriminating objects in a distant scene or driving while in the presence of glare from the sun.
Measures of visual performance are significantly improved with photochromic compared to clear spectacles lenses. It remains to be seen whether a light-adapting contact lens could do the same.
In terms of ameliorating some of these undesirable effects, the use of filters to reduce either overall illumination or specific wavelengths may be helpful. What then are the measures of visual performance that may be affected by selective light filtering?
MEASURES OF VISUAL PERFORMANCE AFFECTED BY LIGHT FILTERING
Glare Glare occurs when luminance, or luminance ratios, are excessively high in relation to the state of adaptation. Glare reduces both contrast sensitivity17 and high- and low-contrast acuity.18 It is categorized by American National Standards Institute/Illuminating Engineering Society (ANSI/IES) RP-1-12 into two types: a temporary impairment of vision is termed “disability” glare, and a transitory irritation caused by light is known as “discomfort” glare. It is common to feel some discomfort in response to glare and, in addition to pupil constriction and squinting, to try to avert the eyes away from the glare source. Typical examples include shielding the eyes from the sun on a bright day or looking away from oncoming headlights when driving at night (Figure 2). Whereas the use of a filter, such as sunglasses, does not change the luminance ratio, visual comfort is improved because overall retinal illumination is reduced. Spectral filtering can help with both types of glare: increasing tolerance in disability glare and increasing the bandwidth of comfortable visual operation in discomfort glare (Table 1).
Figure 2. Examples of glare sources—sunlight and car headlights.
TABLE 1 KEY MEASURES OF VISUAL PERFORMANCE AFFECTED BY LIGHT FILTERING
MEASURE
REAL-WORLD EXAMPLE
Glare (two types)
The discomfort experienced when exposed to bright light (or the temporary visual disability when excess light causes increased intraocular scatter) and reduced contrast for reading road signs on a bright day.
Squint response
Aversion tactic when exposed to an uncomfortable level of light such as bright sunlight.
Starbursts/halos
A spreading of light seen around bright points of light such as car headlights.
Chromatic contrast
Real visual scenes contain chromatic borders. Filtering one border more than another can enhance chromatic edges.
Photostress recovery time
Time taken to recover after being dazzled by bright light.
Visual range
Reduced visual range due to scattering and haze in an outdoor scene.
Squint Response When presented with excessive light, we compensate by squinting to try to reduce the uncomfortable level of light entering the eye. In everyday life, a prolonged need for squinting can lead to discomfort and visual fatigue. Glare causes eyelid squint response along with contraction of the orbicularis oculi.19,20 This response to a glare source is implicated in the sensations of fatigue and discomfort that can be reported under such conditions.3,19 In research, the squint response can be used to measure the reaction to different light sources. Given that squinting occurs in reaction to excess light, it is reasonable to believe that the use of spectral filters would help to reduce the magnitude of the response.
Starbursts/Halos Dysphotopsia is defined as the presence of halos, starbursts, or glare (Figure 3). It is often reported in pseudophakes or post-laser-assisted in situ keratomileusis (LASIK). Age-related changes in the eye increase intraocular light scatter and, in turn, the incidence of dysphotopsia.
Figure 3. Example of starbursts seen with car headlights.
Investigating the visual performance of drivers who had and did not have visual impairment, Ortiz and colleagues found that drivers who had pathology had increased sensation of glare and a perception of larger halos around central lights, which severely diminished their capacity to detect peripheral lights surrounding the central source.21 The researchers felt that this deterioration in visual performance could cause trouble with seeing pedestrians and road signs, thus representing a risk factor in traffic. Given the links with light scatter and glare, it is again reasonable to think that the perception of starbursts and haloes could be reduced with the use of spectral filters.
Chromatic Contrast Picture a black and white scene, in which only luminance varies in the image. This is an example of achromatic contrast. A colored scene will contain differences in chromaticity (Figure 4), which can occur across both space—spatial chromatic contrast—or across time—temporal chromatic contrast.22 Thinking of the scene in Figure 4, spatial contrast varies among the different colors of leaves on the trees, while temporal chromatic contrast may alter discrimination of those colors over time as the ambient light changes throughout the day. Plotting the chromatic CSF shows that at low spatial frequencies, chromatic contrast sensitivity is greater compared to achromatic contrast sensitivity.
Figure 4. Scene illustrating heterochromic contrast.
Conversely, sensitivity is much greater in achromatic contrast for higher spatial frequencies, as illustrated by the extreme far side of the CSF curve at which high-contrast visual acuity using a black-on-white target is measured. Differences also exist between colors, with superior contrast sensitivity for red-green gratings than for blue-yellow gratings. These differences can be used in conjunction with achromatic CSFs to further describe visual performance. Enhancing contrast, including enhancing chromatic contrast via the use of filters, helps improve overall spatial vision through better detection of the edges of objects in a scene.23,24 Just imagine how improved chromatic contrast could help with distinguishing details, such as the blue sky and the green trees, from each other in our example scene (Figure 4).
Photostress Recovery Time Related to glare, photostress is the aftereffect of extreme disability glare. After being exposed to a bright light, the visual system needs time to readjust its adaptive state. Time to recover from photostress has been used as a clinical assessment of visual function. It can enable different pathologies to be differentiated: subjects who had maculopathy had longer recovery times compared to those who had optic nerve disease.25 Sudden vision loss can be debilitating. An everyday example would be the time taken for vision to recover after being dazzled, via disability glare, with car headlights while driving. Spectral filtering can expedite photostress recovery26,27 and, given this real-world example, would potentially be a safety advantage by enabling drivers to regain clear vision more quickly.
Visual Range Due to Light Filtering It has been argued that many objects viewed outdoors result in large amounts of mid- and long-wavelength light.28 These are viewed on backgrounds that are short-wavelength dominant, with the earth’s atmosphere scattering those shorter wavelengths into the typical blue haze of the sky. Blue haze degrades visibility, reducing both how well and how far we see.
Spectral filters can increase visual range by preferentially blocking the scattered blue light associated with haze.28 Increased visual range can enable the resolution of detail in a scene from further away. This could in theory deliver benefits for patients ranging from improved visual discrimination further down the fairway during a golf game through to improved visual performance for airline pilots.
EFFECT OF PHOTOCHROMATIC SPECTACLE LENSES ON VISUAL PERFORMANCE
The principles behind the wide-spread use of photochromic spectacle lenses are sound: to provide adaptive filtering of the varying levels of light that the eye is exposed to on a daily basis. The influence that these lenses have on visual function is less well understood, however.
A recent study examined this area, with measures of visual function carefully chosen to best reflect real-life conditions.29 Disability glare, discomfort glare, chromatic contrast, and photostress recovery time were assessed in 75 healthy adults aged 19 to 73 years (mean = 45.61 ± 13.24 years). Three partially activated photochromic lenses were used with a steady state transmittance of 63% (Gray 1), 71% (Gray 2), and 71% (Brown) and compared with a clear lens of 92% transmittance (polycarbonate). The stimuli used to measure the four visual functions closely matched sources found outdoors, such as the spectra of the xenon light used to assess disability glare and photostress recovery being similar to that of bright sunlight.
Results showed that all visual functions measured were significantly improved for all of the activated photochromic lenses tested versus the clear lens (Table 2). It was concluded that the filtering provided by photochromic lenses significantly increased a subject’s ability to both cope with intense broadband and shortwave lighting conditions and to adapt back to normal after being presented with an intense photostressor.29 By reducing the intensity of light exposure, the retinal photopigments are not bleached as much, resulting in smaller changes in adaptive state and quicker recovery. Importantly, these findings are translatable to real-world situations. For example, when driving at 97 km/hour (60mph), the average reduction in photostress recovery of almost five seconds means that a target can be seen around 145 meters (476 feet) sooner when activated photochromic lenses rather than clear lenses are worn.
TABLE 2 SUMMARY OF THE EFFECT OF PHOTOCHROMIC SPECTACLE LENSES ON VISUAL PERFORMANCE
MEASURE
RESULTS
IMPROVEMENT COMPARED TO CLEAR LENS
Discomfort glare
Significantly improved (p < 0.05) with activated photochromic Gray 1 lens versus clear lens, as quantified by both the squint and subjective responses (p < 0.05).
Around 20% improvement*
Disability glare
Significantly improved (p < 0.05) with activated photochromic lenses tested versus clear lens.
Around 13% to 20% improvement
Photostress recovery time
Significantly reduced (p < 0.05) recovery time with activated photochromic Gray 1 lens as quantified by both the squint and subjective responses (p < 0.05).
Around 33% improvement in recovery time
Chromatic contrast
Significantly improved (p < 0.05) with activated photochromic lenses tested versus clear lens. Improved chromatic contrast indicated when viewed through Gray 1 photochromic lens.
Around 13% to 20% improvement
*Note that this response, as a psychological variable, is non-linear.
Additional work has examined the effect on visual performance with intraocular lenses (IOLs) that contain blue-light filters. When compared to IOLs with no visible blue-light filter, subjects who had blue-light-filtering technology IOLs had significantly reduced disability glare and improved measures of safe driving in a driving simulator.30 The study concluded that functional performance—for example, daytime driving in the presence of glare—can be improved with spectral filtering.30 A separate in-vivo study, using a contralateral comparison of blue-filtering and non-blue-filtering IOLs, established significant improvements in disability glare, heterochromic contrast threshold, and photostress recovery in the eyes with blue-filtering IOLs.27
Whereas the use of filters cannot improve visual acuity, there are many examples of spectral filters in nature, suggesting that they confer an evolutionary advantage.31 In humans, much work has been conducted on the yellow-based macular pigments lutein and zeaxanthin. Screening the foveal cones from short-wave light improves disability glare, chromatic contrast, and photostress recovery.32 These results confirm what is seen in many other species that the use of yellow filters appears to improve many aspects of visual performance.
THE NEXT STEP IN THE EVOLUTION OF CONTACT LENSES
In April 2018, the U.S. Food and Drug Administration (FDA) cleared for use the first contact lens to incorporate an additive that automatically darkens the lens when exposed to bright light. Under partnership with Transitions Optical, Acuvue Oasys with Transitions Light Intelligent Technology (Johnson & Johnson Vision Care, Inc.) will be a first-of-its-kind contact lens to provide wearers with vision correction and a dynamic photochromic filter to help balance the amount of light entering the eye. The lens is due for commercial release in 2019.
CONCLUSION
The total visual experience is influenced by many different factors. Visual acuity provides only one small insight, and, in reality, the dynamic nature of our visual tasks, optical systems, widely varying illumination levels, and visual perception all combine to produce the complete visual experience. It is possible to measure key elements of visual performance that are relevant to everyday life. This allows the performance of corrective optical devices to be quantified and compared.
Photochromic spectacle lenses improve the visual experience across four key measures of visual performance. The year 2019 will see the arrival of a first-of-its-kind photochromic contact lens whose clinical performance remains to be described. CLS
REFERENCES
Cheng X, Maggio T, Johnson B, Pall B, Coles-Brennan C. Life Demands More Than 20/20. Contact Lens Spectrum. 2017 Nov;32:33-35,44.
Jubin P, Buch J, Nankivil D. The Three Dimensions of Vision Satisfaction. Contact Lens Spectrum. 2018 Apr;33:38-42,51.
Buch J, Hofmann G, Ruston D. Getting into Your Comfort Zone. Contact Lens Spectrum. 2018 Jul;33:34-38,40,41.
Owsley C. Contrast sensitivity. Ophthalmol Clin North Am. 2003 Jun;16:171-177.
Arden GB, Jacobson JJ. A simple grating test for contrast sensitivity: preliminary results indicate value in screening for glaucoma. Invest Ophthalmol Vis Sci. 1978 Jan;17:23-32.
Jindra LF, Zemon V. Contrast sensitivity testing: a more complete assessment of vision. J Cataract Refract Surg. 1989 Mar;15:141-148.
Shandiz JH, Nourian A, Hossaini MB, et al. Contrast Sensitivity versus Visual Evoked Potentials in Multiple Sclerosis. J Ophthalmic Vis Res. 2010 Jul;5:175-181.
Lesmes LA, Lu ZL, Baek J, Albright TD. Bayesian adaptive estimation of the contrast sensitivity function: the quick CSF method. J Vis. 2010 Mar 30;10:17.1-21.
Hou F, Lesmes LA, Kim W, et al. Evaluating the performance of the quick CSF method in detecting contrast sensitivity function changes. J Vis. 2016;16(6):18.
Owsley C, Sekuler R, Siemsen D. Contrast sensitivity throughout adulthood. Vision Res. 1983;23(7):689-699.
Kalia A, Lesmes LA, Dorr M, et al. Development of pattern vision following early and extended blindness. Proc Natl Acad Sci U S A. 2014 Feb 4;111:2035-2039.
Cheng X, Moody K, Xu J. Visual performance of silicone hydrogel daily disposable contact lenses. BCLA. Liverpool, UK; 2017.
Craig JP, Willcox MD, Argüeso P, et al. The TFOS International Workshop on Contact Lens Discomfort: report of the contact lens interactions with the tear film subcommittee. Invest Ophthalmol Vis Sci. 2013 Oct 18;54:TFOS123-TFOS156.
Puell MC, Pérez-Carrasco MJ, Palomo-Alvarez C, Antona B, Barrio A. Relationship between halo size and forward light scatter. Br J Ophthalmol. 2014 Oct;98:1389-1392.
Van Den Berg TJ, Van Rijn LJ, Michael R, et al. Straylight effects with aging and lens extraction. Am J Ophthalmol. 2007 Sep;144:358-363.
Harrison JM, Applegate RA, Yates JT, Ballentine C. Contrast sensitivity and disability glare in the middle years. J Opt Am A Opt Image Sci Vis. 1993 Aug;10:1849-1855.
Regan D, Giaschi DE, Fresco BB. Measurement of glare sensitivity in cataract patients using low-contrast letter charts. Ophthalmic Physiol Opt. 1993 Apr;13:115-123.
Gowrisankaran S, Sheedy JE, Hayes JR. Eyelid squint response to asthenopia-inducing conditions. Optom Vis Sci. 2007 Jul;84:611-619.
Sheedy JE, Truong SD, Hayes JR. What are the visual benefits of eyelid squinting? Optom Vis Sci. 2003 Nov;80:740-744.
Ortiz C, Castro JJ, Alarcón A, Soler M, Anera RG. Quantifying age-related differences in visual-discrimination capacity: drivers with and without visual impairment. Appl Ergon. 2013 Jul;44:523-531.
Witzel C, Gegenfurtner K. Chromatic Contrast Sensitivity. In: Luo R (ed), Encyclopedia of Color Science and Technology. Berlin, Heidelberg: Springer Berlin Heidelberg;2014:1-7.
Luria SM. Vision with chromatic filters. Am J Optom Arch Am Acad Optom. 1972 Oct;49:818-829.
Wolffsohn JS, Cochrane AL, Khoo H, Yoshimitsu Y, Wu S. Contrast is enhanced by yellow lenses because of selective reduction of short-wavelength light. Optom Vis Sci. 2000 Feb;77:73-81.
Glaser JS, Savino PJ, Sumers KD, McDonald SA, Knighton RW. The photostress recovery test in the clinical assessment of visual function. Am J Ophthalmol. 1977 Feb;83:255-260.
Hammond BR, Bernstein B, Dong J. The Effect of the AcrySof natural lens on glare disability and photostress. Am J Ophthalmol. 2009 Aug;148:272-276.e2.
Hammond BR Jr., Renzi LM, Sachak S, Brint SF. Contralateral comparison of blue-filtering and non-blue-filtering intraocular lenses: glare disability, heterochromatic contrast, and photostress recovery. Clin Ophthalmol. 2010 Dec;4:1465-1473.
Wooten BR, Hammond BR. Macular pigment: influences on visual acuity and visibility. Prog Retin Eye Res. 2002 Mar;21:225-240.
Renzi-Hammond LM, Hammond BR Jr. The effects of photochromic lenses on visual performance. Clin Exp Optom. 2016 Nov;99:568-574.
Gray R, Perkins SA, Suryakumar R, Neuman B, Maxwell WA. Reduced effect of glare disability on driving performance in patients with blue light-filtering intraocular lenses. J Cataract Refract Surg. 2011 Jan;37:38-44.
Hammond BR Jr. The visual effects of intraocular colored filters. Scientifica (Cairo). 2012;2012:424965.
Hammond BR Jr., Fletcher LM, Elliott JG. Glare disability, photostress recovery, and chromatic contrast: relation to macular pigment and serum lutein and zeaxanthin. Invest Ophthalmol Vis Sci. 2013 Jan 17;54:476-481.
Dr. Hammond is a professor in the Brain and Behavioral Sciences program at the University of Georgia and is the Principal Investigator of the Visual Sciences Laboratory. He is also a consultant to Johnson & Johnson Vision Care, Inc.
Dr. Renzi-Hammond is an assistant professor of Gerontology and is Principal Investigator of the Human Biofactors Laboratory at the University of Georgia.
Dr. Buch is Senior Principal Research Optometrist at Johnson & Johnson Vision Care, Inc.
Dr. Nankivil is Staff Engineer Vision Products at Johnson & Johnson Vision Care, Inc.