


Refitting a Corneal GP Lens Over a Scar
This case is from a long-term, 67-year-old patient who has bilateral keratoconus. He has been wearing corneal GP contact lenses since 1981. He had never previously experienced any adverse events during his many years of contact lens wear.
We instruct all of our patients on how to properly maintain their lenses and also to return for a yearly follow-up visit. However, well-designed and properly fit lenses in the hands of a patient who takes good care of them frequently results in a bit of overconfidence that everything is OK long term; such patients tend to return sometimes after two to three or even more years just to be refit with new lenses.
A few months ago, this patient lost one of his lenses and came for a follow-up visit to obtain a new lens. He was wearing a previous lens with the same parameters, but he noted that he experienced pain and some secretion with both lenses. We found that he had a central scar and mild central epithelial edema adjacent to the central scar. We also observed that there was a small, rounded area with an elevation. The patient was instructed to suspend lens wear, to instill only preservative-free artificial tears, and to let the healing process occur. After one week, the edema was 95% resolved. We also observed tear instability and a low lacrimal meniscus at the lower lid, which may have also contributed to the current condition.
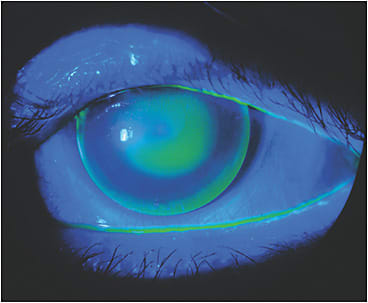
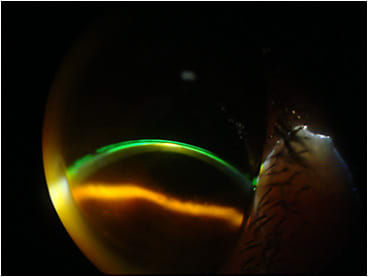
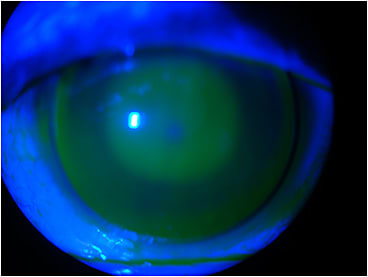
We refit the lens with a steeper central base curve and the same secondary base curve, which seemed to result in a good fit (Figure 1). But a few days later at the first post-new-fit follow-up visit, he still noted moderate discomfort. Re-evaluating the fit in a subsequent slit lamp examination, we observed that there was mild touch of the lens at the apex where the scar produced the small, rounded elevation (Figures 2 and 3).
When my father, Saul Bastos, MD, specialized in contact lens fitting, he used to perform a local, minor thermal procedure at the slit lamp in such cases. He would microcauterize the elevation produced by a scar. He instilled a topical anesthetic drop, then, using cauterization, he would level the elevation at the epithelium. He would then instruct patients to apply medication and lacrimal drops to help the healing process and prevent infection. We still see some of these patients, and they say that this thermal microcauterization procedure helped them return to wearing their GP lenses (“It was a relief.”). I do not believe that such a procedure was ever widespread for this purpose, as the literature refers to the use of thermal microcauterization only in animals (dogs and horses)1 and in human corneal perforations. I suspect that my father brought this idea from his early days of otorhinolaryngology, which he used to practice as well as ophthalmology. Thermal microcauterization is a common procedure in this area.
Rodrigo de Napole, MD, an ophthalmologist at the Fundação Banco de Olhos de Goias (FUBOG), mentioned that with today’s laser technology, superficial phototherapeutic keratectomy2 is performed in such cases. This procedure may not only treat the scar but also remove corneal opacities. There is also a manual treatment option that uses alcohol and mitomycin following keratotomy. These techniques are performed by corneal surgeons in a surgical room. The thermal microcauterization procedure that my father used to do was at the slit lamp, but physicians must have the proper surgical skill to perform this mild procedure.
Management of the Case
The scar and the small, dot-sized corneal opacity did not compromise the visual acuity with a corneal GP lens. Scleral lens fitting would be an excellent way to manage the problem and to vault over the elevation; however, the patient had worn corneal GPs for 27 years, and he preferred to remain in corneal GPs.
His previous GP lens parameters were 58.50D x 45D base curves (BCs), –9.50D power, 9.6mm overall diameter (OAD), 6.5mm optical zone diameter (OZD), and 1.997 sagittal height (sag) (corrected for monovision in nondominant eye). We first changed the base curves to 59D x 45D (Figure 3), but it was not enough to clear the scar. The new lens that we designed had parameters of 60D x 46D BCs, –12.50D, 9.8mm OAD, 6.8mm OZD, and 2.187 sag, with a slighter increase in the optical zone (Figure 4). We decided, with the patient, to improve his distance vision, and he is still able to read J2 without reading glasses.
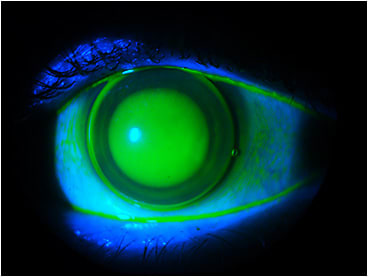
This case demonstrates an interesting aspect in recent corneal GP fitting that we have done. In some specific cases, we are utilizing the sag value for corneal GP fitting. This is the same concept used in customizing scleral lens fitting—adapting the different zones and curvatures in a way to obtain the best possible alignment to the ocular surface. Here, we augmented the sag utilizing a combination of a steeper central base, a steeper secondary base curve, and also a slight increase in the central optical zone. This induced greater pooling and was steep enough to vault the elevation obstacle while preventing the formation of microbubbles. Visual acuity was not affected due to the greater pooling of the steeper lens.
Discussion
In cases such as this with corneal scars and altered epithelium, we have a few options to resolve the fitting. It is important to understand that even with scleral lenses, which seem to be a healthy option for patients who have this condition, the fit may be compromised if the lens is too close to the cornea. Another option is to refer patients to a corneal surgeon for treatment, be it manual or with a laser.
We resolved this issue by fitting a steeper corneal GP design—increasing the sag and managing each curve and zone to make the lens steep enough to vault the scar while preserving tear exchange and centration and, especially, not inducing microbubbles.
Conclusion
Working with sag values in corneal GPs is similar to working with them in scleral lenses, but it is important to understand that the magnitude of the change in microns is significantly smaller compared to with scleral lens fitting. Be sure to examine the fitting using all resources, especially slit lamp observation with fluorescein and cobalt blue illumination, both frontal and at 45º with a thin slit light. I strongly recommend capturing these images for posterior examination on a large screen. This way, you can take the time needed to plan the changes that you believe will result in the desirable effect. Remember that challenging cases frequently need one or more attempts to acquire the best possible fitting. We usually charge a higher fee in these cases, always making sure that the patients understand the difficulty of the case.
I believe that most GP lens manufacturers do not include sag values for their corneal GPs, but it may be possible to do so because most GP design software has that information. I hope that this case may help those corneal GP and scleral lens fitters who often are exposed to challenging cases and feel that they would like to try something different toward improving the fit.
References
- Bentley E, Murphy CJ. Thermal cautery of the cornea for treatment of spontaneous chronic corneal epithelial defects in dogs and horses. J Am Vet Med Assoc. 2004 Jan 15;22:250-253,224.
- Rathi VM, Sharadini PV, Sangwan VS. Phototherapeutic keratectomy. Indian J Ophthalmol. 2012 Jan-Feb;60:5–14. Available at www.ncbi.nlm.nih.gov/pmc/articles/PMC3263247 . Accessed on Dec. 5, 2018.