


A 67-year-old female presented for evaluation. Her primary complaint was persistent epiphora, which began four days earlier. While working in her garden, she leaned over a cactus plant, which “scratched” her left eye. She reported mild foreign body sensation, but no actual pain. The epiphora, which began immediately after the injury and had persisted for the entire four-day period, was very bothersome and annoying.
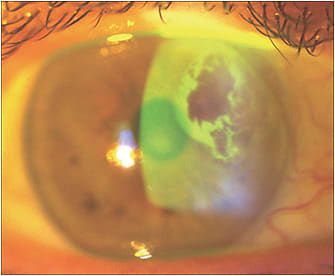
Best-corrected visual acuities were OD 20/20 and OS 20/25. Biomicroscopy revealed bilateral nuclear sclerosis cataracts. After sodium fluorescein was instilled onto the ocular surface OD and OS, we noted a typical tear film pattern OD. The tear film pattern OS was unusual, with concentric, variable degrees of brightness as evident in the image. Intraocular pressures were OD 12 mmHg and OS 16 mmHg.
Further examination revealed a minute, full-thickness perforation of the cornea; a similar injury to the anterior surface of the iris was perfectly aligned with the corneal injury. No cells or flare were noted in the anterior chamber. Dilated examination revealed that there was no penetrating injury to the lens capsule.
Our initial diagnosis was penetrating injury of the cornea and iris, with no apparent infection or inflammation. The inequality of IOP between the two eyes was explained by the unrestricted loss of aqueous through the corneal perforation. After instilling a topical antibiotic, we applied a bandage contact lens, primarily for the purpose of reducing aqueous outflow though the corneal break. We also prescribed a topical antibiotic to be used in conjunction with the bandage lens. One week later, the wound was completely closed, and the anterior chamber was quiet.
Any penetrating corneal injury has the potential to cause endophthalmitis. Lu et al reported Pseudomonas aeruginosa endophthalmitis secondary to an accidental injury with a hypodermic needle.1 After performing an in-office procedure to remove a foreign body from the cornea, an ophthalmologist irrigating the eye accidently dropped a syringe and needle that penetrated the cornea. The patient subsequently developed a severe Pseudomonas endophthalmitis.
In our case, the patient was very fortunate not to have developed endophthalmitis. Factors that possibly contributed to avoidance of endophthalmitis include continuous outflow of aqueous, which prevented microbe ingress into the globe, and the very dry climate. In penetrating ocular injuries, the prognosis for a good visual outcome is influenced by several factors including severity of the initial penetrating injury.2 Other factors that influence final visual outcome include initial visual acuity and presence of an afferent pupillary defect as well as of infection.2
Geographic location also influences the most likely pathogen and final outcome of corneal ulcers. In the United States, gram-positive bacteria are the predominant causative organisms in temperate and northern locations; in the South, gram-negative organisms are more commonly cultured from bacterial ulcers.3
In vegetation-related infectious keratitis, fungi must be considered in the differential. Estopinal et al reported a higher incidence of bacterial keratitis in all regions except for the southeastern United States, where fungal infectious keratitis dominates.3
Dr. Townsend practices in Canyon, Texas. He is treasurer of the Ocular Surface Society of Optometry. He is also a consultant or advisor to Alcon, Allergan, NovaBay, Odyssey Medical, ScienceBased Health, Shire, and TearLab. Contact him at drbilltownsend@gmail.com.
References
- Lu C, Hao JL, Liu XF, Liang LL, Zhou DD. Pseudomonas aeruginosa endophthalmitis caused by accidental iatrogenic ocular injury with a hypodermic needle. J Int Med Res. 2017 Apr;45:882-885.
- Phogat JK, Gagneja V, Sachdeva S, Rathi M. Evaluation of a Case of Penetrating Ocular Injury. Indian Journal of Clinical Practice. 2012 Jun;24:62-64.
- Estopinal CB, Ewald MD. Geographic Disparities in the Etiology of Bacterial and Fungal Keratitis in the United States of America. Semin Ophthalmol. 2016;31(4):345-352.