



At a recent research conference, an academic colleague corrected my comment on accommodation with “it’s not accommodation; it’s near refractive state.” This distinction has stuck with me. When termed “accommodation,” it’s easy for practitioners to bundle this important measure of their patients’ visual function into the binocular vision basket—consigning its relevance to children’s vision assessments and not to primary care or general contact lens practice. However, when practitioners think of accommodation as the “near refractive state,” it compels them to put as much effort into getting it right, and for a wider range of patients, as they do the distance refractive state.
Practitioners understand the importance of getting the add power correct for their presbyopic patients, especially in multifocal contact lens wear. Accommodative insufficiency has been shown to be the primary driver of symptoms in children who have convergence insufficiency, a condition with a wealth of evidence-based data for diagnosis and treatment (Scheiman et al, 2006).
Alongside the relevance of binocular vision function to visual comfort in patients of all ages, and in conjunction with increased prescribing of multi-zone and multifocal contact lenses to young myopes, there is increasing research interest in understanding how these patients will use these lenses at near; this is notable considering that many of these designs were originally created for presbyopes. What else could you be doing to understand the near refractive state of your younger contact lens-wearing patients and how this could influence comfort, satisfaction, and efficacy?
Spectacles to Contact Lenses at Near
When hyperopes wearing spectacles look at a near target, their convergence away from the optical center of the lenses creates base-out prism in each eye, which moves the image inward and, therefore, decreases the convergence demand. When hyperopes then switch to contact lens wear, they have to converge more by themselves, which will result in an esophoric shift. In addition, the increased effective prescription of a plus-powered single-vision distance contact lens (SVD CL) compared to a spectacle lens allows hyperopic CL wearers to reduce their accommodative effort compared to spectacle wear (Bennett and Rabbetts, 1989) (Figure 1).
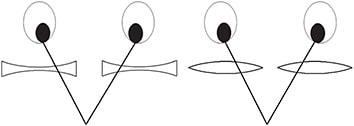
In contrast to hyperopes, myopes reading through their spectacles experience base-in prism at near, moving the image further away (Figure 1). Looking away from the optical center of the lens also reduces the power, effectively reducing the accommodative demand. When myopes change to SVD CLs, they must increase their accommodation, which is why early presbyopic, moderate-to-high myopes always need an add in their contact lenses before they need it in their spectacles. And, high myopes can sometimes survive presbyopia without ever needing progressive spectacles. Myopes of any age must increase accommodation demand in an SVD CL correction; they will show an exophoric shift in contact lenses as they lose the base-in spectacle correction (Hunt et al, 2006). This can be beneficial to moderate-to-high myopes who have esophoria in spectacles, in which the spectacle-to-contact-lens effect will be greater and given that esophoria at near has been associated with a higher rate of myopia progression in SVD spectacles (Yang et al, 2009).
These theoretical calculations have been confirmed experimentally in young adult CL wearers; the differential between spectacle and CL binocular vision function at near generally increases with increasing CL power, with individual variation (Hunt et al, 2006).
Binocular vision (BV) disorders can cause asthenopia (Rouse et al, 2009); interestingly, they have also been linked to dry eye. Researchers investigating the relationship between contact lens-induced dry eye symptoms and BV disorders found a significant correlation between severity of symptoms on the Ocular Surface Disease Index (OSDI) survey and the Convergence Insufficiency Symptom Survey (CISS). Young myopic soft contact lens wearers also had a 48% frequency of a BV disorder, with the most common being accommodative lag of 1.0D or more. The authors recommended that clinicians screen symptomatic contact lens-wearing dry eye patients for BV disorders, as the overlap of these symptoms could lead practitioners to confuse the diagnosis of one for the other (Rueff et al, 2015).
Up Close—the Next Frontier in Myopia Research?
Myopia has long been associated with inaccurate and insufficient accommodative behavior at near and increased accommodative convergence in comparison to emmetropes (Gwiazda et al, 1995; Charman, 1999; Drobe and de Saint-André, 1995; Gwiazda et al, 2005; and others. Full list available at www.clspectrum.com/references ). The impact of orthokeratology (OK) and multifocal contact lenses (MFCLs) on near refractive state is pertinent to both visual comfort and to understanding mechanisms of myopia control. Esophoria and accommodative lag have been shown to improve in multifocal (Tarrant et al, 2008; Aller et al, 2016; Gong et al, 2017; Kang et al, 2016) and in OK contact lens wear (Gifford et al, 2017a; Gifford et al, 2017b; Tarrant et al, 2009), although not as may be predicted by the labelled add power of an MFCL or central refractive power of the OK treatment. Two key research papers are relevant to how binocular vision function could help “power up” the efficacy of these CL corrections.
First, fitting bifocal soft contact lenses to myopic children who have esophoria at near, in which the add was chosen to neutralize the associated phoria, resulted in a 70% reduction in axial elongation over 12 months compared to single-vision soft CL-wearing controls (Aller et al, 2016). This is an impressively high result compared to the average 30% to 50% seen in other similar studies (Huang et al, 2016).
Second, in a two-year study, children who had lower baseline accommodative amplitude showed a 56% better myopia control response to OK lens wear compared to normal accommodators (Zhu et al, 2014). In this study, the researchers separated the children by mean accommodative amplitude into “below average” and “above average” accommodators. The children who had “below average” accommodation showed a bigger improvement in their amplitude in OK wear (around 4.0D more, compared to around 1.0D for the “above average” accommodators) and a better myopia control effect.
How children accommodate through an MFCL could influence their efficacy for myopia control. Some studies have shown that children accommodate normally through these lenses (Anstice et al, 2011), while other studies have shown that children and young adults may alternately relax their accommodation and use the add of the lens at near (Gong et al, 2017; Kang et al, 2016). Answering this question could help to achieve consistent or better efficacy of these treatments.
Monocular modeling of optical quality through multifocal lenses has shown that smaller central distance optical zones (such as in a presbyopic MFCL design) could lead to young wearers “using” the add at near, resulting in hyperopic defocus from the distance portions of the lens both centrally and peripherally; this is presumably a deleterious outcome for myopia control. This modeling also showed that larger central distance optical zones (such as in OK) could encourage a normal accommodation, giving myopic defocus from the add portions of the lens, which is a presumed goal of myopia control (Faria-Ribeiro et al, 2018).
Perhaps in the future, we will have a measure, or a combination of measures, of accommodation and binocular vision to help practitioners pick the best lens design for individual patients; normal accommodators could get one type of lens, while below average accommodators could get a different type. It’s likely that one single add—as employed by some myopia controlling soft lenses—won’t give practitioners everything that they need to bridge the gap to an efficacy higher than the average 50% generally seen in contact lens corrections (Sun et al, 2015; Li et al, 2017).
In Summary
It is important to understand binocular vision status in spectacle wear prior to contact lens fitting, as the optical impact of this change could lead to significant symptoms, or even significant improvement of symptoms, in particular patients. Furthermore, understanding binocular vision status—particularly the presence of accommodative lag—could provide effective insights into diagnosis and management of contact lens-induced dry eye in non-presbyopic patients. Finally, measuring accommodation function could provide the future mechanisms to improving efficacy of contact lenses fit for myopia control. CLS
For references, please visit www.clspectrum.com/references and click on document #276.