



A practitioner’s ability to modify a parameter of the GP portion of a hybrid contact lens has historically been limited. Alterations to the GP base curve to improve fitting relationship of the hybrid lens on eye is routine. In cases in which practitioners use this modality for the management of presbyopia, what modifications can be made beyond improvement of the fit on eye to optimize quality of vision experienced by a wearer?
If practitioners consider the aspheric GP optics of progressive hybrid lens designs available for clinical use today, there are two categories to explore—center-near and, more recently, center-distance progressive zone options. Although some movement is observed when fitting these contact lenses, the soft skirt of a hybrid lens essentially maintains the same position on eye throughout wear. Because practitioners cannot rely on optimal optics to move into position in front of the pupil depending on target viewed, they need to focus on the dynamics of the pupil to best utilize the optics in front of it.
Adjust to the Pupil
Small A small measured photopic pupil size (2.5mm), typical in mature presbyopes, would likely do best in a center-near design (Figure 1A). Hybrid lenses are not designed to translate upon blink, and the increased visual demands at near for this population would warrant a compact near progressive zone to cater to the small window of vision.
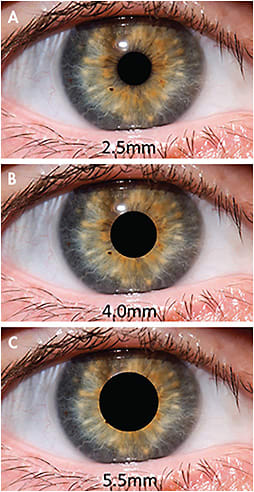
Mid-range Figure 1B shows a mid-range measured pupil size (4.0mm) under photopic lighting conditions. The pupil often retains enough dynamic properties to allow it to dilate past the progressive center-near transition zone in dim lighting to maximize distance viewing.
A method to troubleshoot poor distance viewing for such an eye is to fit a center-distance design with alterations to the size of the transition zone to best suit the visual needs of this patient.
Large Figure 1C shows a large photopic pupil size that can be found in emerging presbyopes. This type of eye is more sensitive to decreases in vision due in part to the larger amount of light that can enter the eye. Regardless of the size of the near zone selected, a center-near lens would have a significant amount of visual information going through the pupil from near viewing and will likely not yield a happy patient.
There are still some progressive benefits for such patients when one eye, usually the dominant eye, is fit with a center-distance lens and the progressive zone is designed to be typically smaller than the photopic pupil size. This type of modified monovision can benefit some of the most visually taxing patients for distance-related tasks, while still allowing some of their near viewing demands to be met. CLS