



A 62-year-old male patient had undergone bilateral four-incision radial (RK) and astigmatic-correcting arcuate keratotomies (AK) back in 1995. He did very well postoperatively, with uncorrected visual acuities of 20/20 in both eyes. However, two weeks later, he suffered a foreign body injury to his left eye (a wooden chip) that re-opened the temporal arcuate incision. Since the injury, he has experienced a continual loss of uncorrected visual acuity in the left eye only.
Today, his uncorrected visual acuities are OD 20/20 and OS 20/60. Simulated keratometric readings are OD 42.00/42.62 (0.62D corneal toricity) and OS 39.25/45.75 (6.50D corneal toricity). Anterior segment optical coherence tomography (AS-OCT) imaging showed a significant amount of wound gape and scar tissue at the site of the temporal arcuate incision. The scarring went down to approximately three-quarters of the corneal thickness (Figure 1).
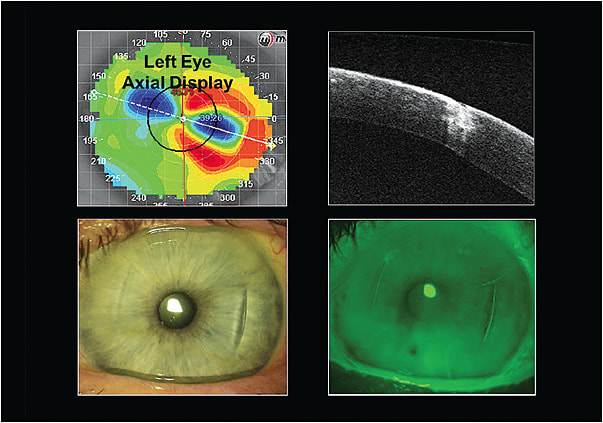
Wound Gape
In 1983, Rowsey described the 10 topographical “rules” associated with incisional keratotomies. He stated that as radial and/or arcuate incisions are placed into the paracentral and peripheral cornea, the unsutured wounds gape. The amount of wound gape and the subsequent corneal flattening will be influenced by a number of biological and surgical factors that include patient age at the time of surgery; number, length, and depth of the incisions; preoperative shape factor; individual wound healing response; and stresses and biochemical properties within the corneal tissue.
These tissue stresses or “push/pull forces” within the cornea occur posteriorly by intraocular pressure (IOP) as well as radially and circumferentially (Figure 2). Together, they are responsible for three primary topographical findings: 1) All corneal incisions or lacerations flatten the cornea over the site of the incision (trauma) as well as 90º away; 2) The corneal flattening effect is greatest as the incision or laceration approaches the visual axis; 3) The greater the amount of wound gape, the greater the amount of corneal flattening.
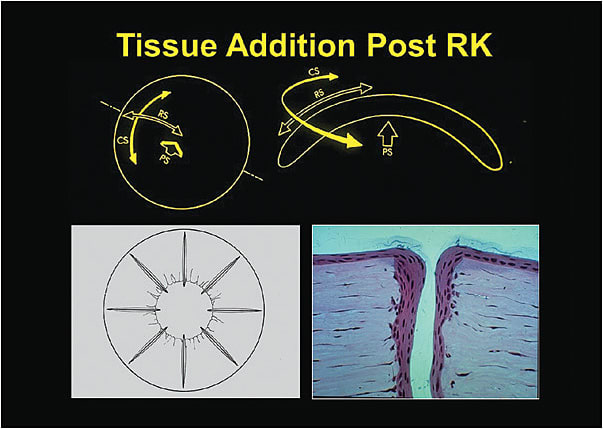
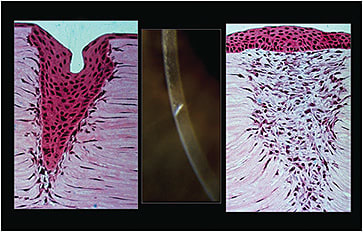
The first response to any surgically placed radial and/or arcuate incision is the presence of epithelium migrating down the “walls” of the incision, resulting in an epithelial plug. With time, the plug is pushed out and replaced by scar tissue that increases the corneal surface area. The radial incision creates a diffuse corneal flattening that is greatest in the center of the cornea, and the astigmatic-correcting arcuate incisions selectively flatten the cornea along the steep corneal meridian (Figure 3). The patient’s left eye was eventually fitted with a scleral lens, and he achieved a best-corrected visual acuity of 20/20. CLS
The authors would like to thank Dr. Emily Cheng for her assistance with this Case Report.
For references, please visit www.clspectrum.com/references and click on document #274.