



For the sixth consecutive year, the American Optometric Association (AOA) Contact Lens & Cornea Section (CLCS) presented a two-hour course on the topic of “Clinical Controversies” at Optometry’s Meeting, which took place in June in Denver. The focus of the 2018 Clinical Controversies program was two-fold: 1) Myopia Management, and 2) Controversies in Advocacy. The latter topic, presented by CLCS Past Chair Dr. Jeff Sonsino, will be published as a separate article.
An audience response system was used to poll eye-care practitioners (ECPs) in attendance about their preferences as they pertained to the various corrections. This system was coordinated by former American Optometric Student Association national liaison to the CLCS, Dr. Taylor Little. Many of these responses are included in this article.
THE DISEASE OF MYOPIA
For years, myopia was considered a refractive error. Based on the latest scientific research, myopia is currently defined as a disease or a risk factor for disease. There are three types of myopia: pathologic myopia, school-age myopia, and adult-onset myopia.1 Pathologic myopia occurs before age 6 and is defined as an abnormal and extreme elongation of the axial length of the eye that does not change. School-age myopia occurs between 6 to 18 years of age, with stabilization expected by the late teens to early 20s. School-age myopia is associated with higher IQ scores, extra time reading, and reduced exposure to sunlight compared to non-myopic patients, and it is more common in urban and industrialized countries. Adult-onset myopia appears in adults. An early adult is considered 20 to 40 years old; a late adult is older than 40 years old. This type of myopia is affected by accommodative anomalies and near-vision-dominated occupations. To control myopia, the rate of eye growth must be slowed, which normally occurs naturally at around age 16.2,3
Research indicates that myopia is an independent risk factor for glaucoma, cataracts, choroidal neovascular membranes, and retinal detachment. In pathological myopia, there is a three times greater risk for early onset cataracts, an eight times greater risk for myopic macular degeneration and for retinal holes and tears, and an 18 times greater risk for glaucoma.4
Significantly, the higher the myopia, the higher the risk. Myopia affects 1.6 billion people worldwide, and greater than 80% of the population in Hong Kong, Taiwan, and Singapore is myopic.5 In the United States, 42% of the total population and 25% of children are myopic.5 The prevalence of myopia is rapidly increasing, and it is estimated that 50% of the population will be myopic by 2050.5 Researchers have affirmed that there is no safe level of myopia. Risk factors for myopia include race, genetics, parents with myopia, the environment, time performing near work, and time spent outdoors. Additionally, through genome-wide linkage analysis, a mutation in exon 10 of the gene LEPREL1 has been shown to cause myopia.6
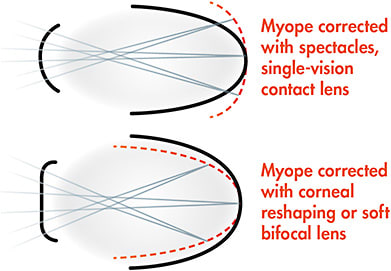
Conventional myopia correction may induce peripheral hyperopia. Peripheral hyperopia, otherwise known as peripheral hyperopic defocus, occurs when peripheral vision is focused behind the retina, regardless of the location of central focus.1 The peripheral retinal area is much larger compared to the central area, and it may be more important to regulating eye growth. When minus lenses focus light at the center of the retina for clear vision, peripheral light rays at the edge of the eye are focused behind the retina. This may re-establish a growth signal and lead to the lengthening of the eye.1-3 Research has suggested that hyperopic defocus on the peripheral retina may be a risk factor for myopia.7 Uncorrected myopic eyes exhibit hyperopic relative peripheral refraction (RPR) in the horizontal ocular meridian. Uncorrected hyperopic eyes typically exhibit myopic RPR.8,9 Changes in myopia progression have been reported from studies of spectacle or contact lens correction that result in large changes in retinal defocus.
With this knowledge that hyperopic defocus is a potential risk for myopia, several methods have been devised to reduce the peripheral hyperopic defocus with the intent to reduce the progression of myopia. Myopic defocus occurs when peripheral light rays beyond the macular region focus in front of the retina. This defocus would encourage the retina to stabilize and not elongate.10 Axial elongation can be controlled with myopic defocus (Figure 1). Both soft multifocal contact lenses and orthokeratology can be used to create a clear image at the macula and to provide myopic defocus on the peripheral retina.
In the Avon Longitudinal Study of Parents and Children (ALSPAC) of 2,833 participants aged 2 to 15 years old, greater time outdoors was associated with a reduced risk of incident myopia from age 3 onward. Additional time outdoors from 3 to 9 years of age was associated with a reduced incidence of myopia between ages 10 to 15.11
There are several theories as to why time outdoors reduces the incidence of myopia. According to multiple human and animal model studies of myopia, it is actual light exposure, not just a decrease in reading time, that decreases the incidence of myopia.12 One theory suggests that exercise is protective and that when children are outdoors, they exercise more. Another theory is that direct light exposure releases vitamin D, which may inhibit eye growth and the onset of myopia.12 A different theory is that light is brighter outdoors and slows abnormal eye growth.12 Yet another postulation is that pupil constriction in brighter light may result in a greater depth of focus. The prevailing theory is that bright outdoor light stimulates a release of dopamine from specialized cells in the retina. Dopamine then initiates a molecular signaling cascade that concludes with normal eye growth, without the development of myopia.12
The most common methods used in practice today in an effort to slow myopia progression include orthokeratology, center-distance multifocal soft contact lenses, pharmaceutical agents (notably atropine), or some combination of these methods.
THE CASE FOR ORTHOKERATOLOGY
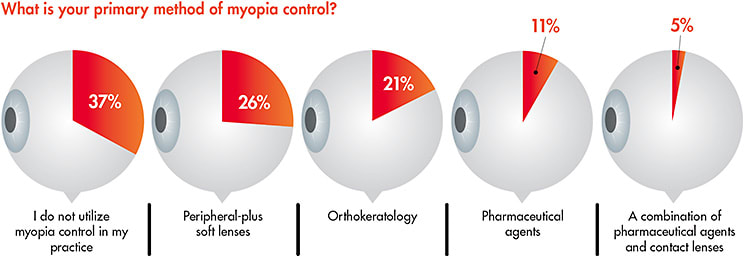
The audience was polled as to their primary method of myopia control (Figure 2). It is evident that peripheral-plus-power soft lens use for this purpose has been growing in recent years, and these results are consistent with those of a recent ECP poll.13
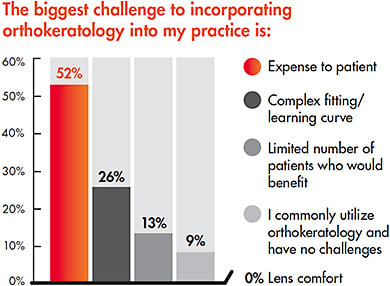
Why orthokeratology is not dominating the myopia control/management arena today—and the fact that a high percentage of practices have not embraced this modality—was posed to the audience. Specifically, they were asked what was the biggest challenge to incorporating orthokeratology into their practice (Figure 3). It is evident that the expense to the patient is of foremost concern, followed by the perception of a complex fitting system with a lengthy learning curve. Interestingly, initial comfort was not an issue; reasons for this could include that orthokeratology lenses have larger diameters compared to conventional corneal GPs in combination with a low edge clearance design and that they are only worn overnight. It is important to note that in recent years, orthokeratology manufacturers have streamlined the fitting of these lenses by providing online certification, simplified fitting and troubleshooting cards, and the ability to successfully fit these lenses empirically. In fact, a nationwide, multi-center study determined that the first-fit success with empirically designed orthokeratology lenses was greater than 80%.14
Orthokeratology offers numerous benefits, notably for young myopic patients. Walline et al15 reported that children as young as 8 years of age can successfully handle GP lenses. Specifically, young progressive myopes only need to wear these lenses at night. If early on in their myopia progression, the corneal reshaping process can result in an emmetropic-to-low hyperopic error in the morning, preventing the need for any vision correction device during the day. This is ideal for young athletes, especially swimmers. Individuals who have less than 5.00D of myopia in combination with less than 2.00D of with-the-rule corneal astigmatism, and who have a small-to-medium pupil size, are most likely to be successful. It is important to avoid fitting individuals who have large pupils with orthokeratology because these designs have small central treatment zones, often 5mm to 6mm; patients who have large pupils will likely experience glare around lights when not wearing the lenses.
Orthokeratology also offers the benefit of slowing the progression of eye growth. The mechanism appears to be the ability of the lens design—which incorporates a reverse curve or a related paracentral/midperipheral steepening—to create a myopic defocus; as discussed previously, this process signals a reduction in axial length progression. According to Walline,16 the amount of reduction is, on average, almost 45%.
Concern has been expressed about orthokeratology with regard to the risk of microbial keratitis. However, recent studies have concluded that the risk of microbial keratitis is no greater with orthokeratology than it is with extended wear in general.17,18
THE CASE FOR PERIPHERAL-PLUS-POWER SOFT LENSES
The soft multifocal peripheral-plus contact lens method of treatment is becoming more popular with the advent of new lens designs. One study showed that 50% to 55% of axial length elongation can be controlled with soft multifocal lenses over the course of treatment.19 It is important to remember that myopia progression is not linear, nor is myopia control.
A concentric ring design will result in a greater reduction in axial length elongation compared to a gradient or aspheric design, at 44.4% and only 31.6%, respectively.20 Center-distance designs may provide the best mechanism of action for controlling myopia with multifocal contact lenses.21 Other designs have been studied, but when we polled the audience, 95% of respondents chose a center-distance design (Figure 4).
A few tips are helpful when fitting a patient with these lenses. Push the maximum amount of add power that is tolerable. The ideal amount would be a +2.50D add.22 If this add power creates central blur, eye strain, or discomfort, the suggested approach would be to first add more minus to the spherical power of the lens before reducing the add power. This treatment is most effective when the add power is placed within the center of the pupil. A patient who has small pupils may not achieve as much of the treatment effect as would someone who has larger pupils and is able to have the full add effect placed within the pupil.19
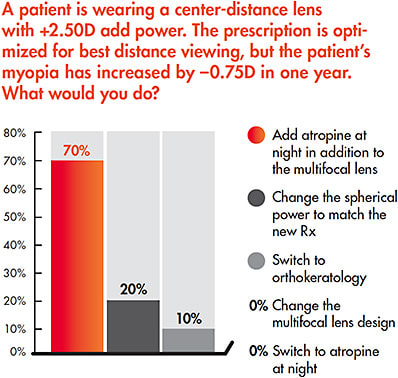
If a patient is fit with center-distance multifocal lenses and progression of myopia continues, there are several available courses of action. The spherical component of the lens design can be adjusted, with continued monitoring of progression. This was a somewhat popular choice among our audience, with 20% of respondents choosing this option when polled (Figure 5). A second option would be to switch to orthokeratology. Only 10% of our audience chose this option because the mechanism of action is the same as with multifocal lenses. With the ability to customize these lenses, more of the add power can be placed within the pupil to potentially achieve a greater magnitude of control. A third option would be a combination treatment: add atropine to the routine. Atropine’s mode of action is different from that of soft multifocal lenses, and the use of both can have a greater impact compared to either on their own.23 This was the most popular choice among our audience, with 70% percent of our respondents choosing this option.
As multifocal lens design development continues and new products enter the market, the possibility of switching designs will increasingly become an option. One such lens that is not yet available in the United States was designed specifically for myopia control. It is a daily disposable lens in a concentric-ring, center-distance multifocal design. The concentric rings alternate between distance correction and a +2.00D add power. There are a total of four rings—two corrective and two treatment rings—in this design.
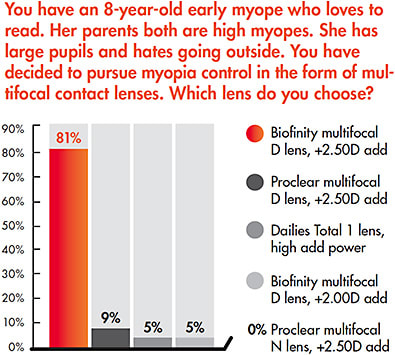
Another daily disposable lens option is available in the United States and is indicated to treat presbyopia. It is an extended depth of focus multifocal lens design that has center-distance optics with up to a +3.00D add power placed immediately next to the central distance zone. This creates a blur zone that is suppressed by the visual cortex, creating a virtual aperture or pinhole on the retina. This technology takes advantage of the depth of focus that is created at the retina. As a result, greater stereopsis and depth perception can be achieved with this lens. In a retrospective case series analysis of 32 patients (ages 6 to 19 years) from 10 practices, approximately 98.4% of the children demonstrated a reduction of annualized myopia progression, with 91% showing a decrease of 70% or greater.24 Overall, 81.25% had complete halting of myopia progression, including myopia regression in 6.25% of the patients. How this lens will impact myopia control is still yet to be studied.
The bottom line is, quoting Professor Brien Holden, “We should fit every myopic child, young adult, and university student with peripheral plus power lenses.”25
THE CASE FOR ATROPINE
Atropine is a non-selective anti-muscarinic receptor agent that has affinity for all five subtypes of muscarinic acetylcholine M1 to M5 receptors. Atropine sulfate is the sulfate salt of atropine, which is derived from the leaves of Atropa belladonna. Atropine consists of an organic base (tropine) and an aromatic (tropic) acid to complete the structure of an organic ester.
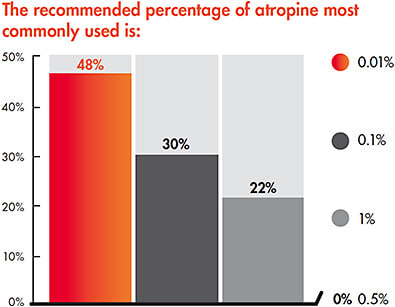
Initially, higher concentrations of atropine (most commonly 1%) demonstrated efficacy in slowing axial elongation from 70% up to 94% in well-conducted trials.26-31 Once lower concentrations of atropine were introduced, fewer side effects and less rebound myopia were reported. With atropine 0.01%, myopia was slowed at a rate similar to atropine 1%, with a negligible effect on accommodation and pupil size.32 Studies suggest that the most effective myopia control options are pharmacologic.33 Low-dose atropine provides an average of 50% reduction of myopia.33 The Clinical Controversies audience was asked what percentage of atropine was most commonly used. The majority of participants responded, not surprisingly, with their preference for 0.01% atropine (Figure 6).
SUMMARY
It is evident that several viable options are available today for slowing myopia progression and eye growth. It is also evident that all of these methods are currently considered off-label applications for myopia control by the U.S. Food and Drug Administration. That said, the future looks promising for the development of contact lenses and pharmaceutical agents that will result in even more slowing of myopia progression. The day is approaching when we should, in fact, offer one (or a combination) of these options to every young emerging myope. CLS
The authors would like to acknowledge Taylor Little, OD, for her assistance with the figures used in this article.
REFERENCES
- Gifford P, Gifford KL. The Future of Myopia Control Contact Lenses. Optom Vis Sci. 2016 Apr;93:336-343.
- Smith EL 3rd, Kee CS, Ramamirtham R, Qiao-Grider Y, Hung LF. Peripheral vision can influence eye growth and refractive development in infant monkeys. Invest Ophthalmol Vis Sci. 2005 Nov;46:3965-3972.
- Cooper J, Schulman E, Jamal N. Current status on the development and treatment of myopia. Optometry. 2012 May 31;83:179-199.
- Tano Y. Pathologic myopia: where are we now? Am J Ophthalmol. 2002 Nov;134:645-660.
- Holden B, Fricke T, Wilson D, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016 May;123:1036-1042.
- Mordechai S, Gradstein L, Pasanen A, et al. High myopia caused by a mutation in LEPREL1, encoding prolyl 3-hydroxylase 2. Am J Hum Genet. 2011 Sep 9;89:438-445.
- Hoogerheide J, Rempt F, Hoogenboom WP. Acquired myopia in young pilots. Ophthalmologica. 1971;163(4):209-215.
- Atchison DA, Pritchard N, Schmid KL. Peripheral refraction along the horizontal and vertical visual fields in myopia. Vision Res. 2006 Apr;46:1450-1458.
- Mutti DO, Hayes JR, Mitchell GL, et al. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2007 Jun;48:2510-2519.
- Smith EL 3rd, Kee CS, Ramamirtham R, Qiao-Grider Y, Hung LF. Peripheral vision can influence eye growth and refractive development in infant monkeys. Invest Ophthalmol Vis Sci. 2005 Nov;46:3965-3972.
- Shah RL, Huang Y, Guggenheim JA, Williams C. Time Outdoors at Specific Ages During Early Childhood and the Risk of Incident Myopia. Invest Ophthalmol Vis Sci. 2017 Feb 1;58:1158-1166.
- Zadnik, K, Mutti D. Why your kids might be able to see better if they play outdoors more often. The Conversation. Sept. 25, 2017. Available at http://theconversation.com/why-your-kids-might-be-able-to-see-better-if-they-play-outdoors-more-often-83693 .
- Bennett ES. GP Annual Report 2018. Contact Lens Spectrum. 2018 Oct;33:20,21,23-25,27-29,50.
- Eiden SB, Davis RL, Bennett ES, DeKinder JO. The SMART Study: Background, Rationale, and Baseline Results. Contact Lens Spectrum. 2009 Oct;24:24-28,30,31.
- Walline JJ, Jones LA, Mutti DO, Zadnik K. A randomized trial of the effects of rigid contact lenses on myopia progression. Arch Ophthalmol. 2004 Dec;122:1760-1766.
- Walline JJ. Myopia Control. In Bennett ES, Henry VA. Clinical Manual of Contact Lenses (5th ed.), Philadelphia, Wolters Kluwer. In Press.
- Bullimore MA, Sinnott LT, Jones-Jordan LA. The risk of microbial keratitis with overnight corneal reshaping lenses. Optom Vis Sci. 2013 Sep;90:937-944.
- Liu YM, Xie P. The Safety of Orthokeratology – A Systematic Review. Eye Contact Lens. 2016 Jan;42:35-42.
- Michaud L, Simard P, Marcotte-Collard R. Defining a Strategy for Myopia Control. Contact Lens Spectrum. 2016;31:36-42.
- Li SM, Kang MT, Wu SS, et al. Studies using concentric ring bifocal and peripheral add multifocal contact lenses to slow myopia progression in school-aged children: a meta-analysis. Ophthalmic Physiol Opt. 2017 Jan;37:51-59.
- Dinardo A, Rosen C. A Bright View of Soft Multifocal Contact Lens Optics. Contact Lens Spectrum. 2017;32:28-32.
- Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Multifocal contact lens myopia control. Optom Vis Sci. 2013 Nov;90:1207-1214.
- Kinoshita N, Konno Y, Hamada N, Kanda Y, Shimmura-Tomita M, Kakehashi A. Additive effects of orthokeratology and atropine 0.01% ophthalmic solution in slowing axial elongation in children with myopia: first year results. Jpn J Ophthalmol. 2018 Sep;62:544-553.
- Cooper J, O’Connor B, Watanabe R, et al. Case Series Analysis of Myopic Progression Control with a Unique Extended Depth of Focus Multifocal Contact Lens. Eye Contact Lens. 2018 Sep;44:e16-e24.
- Holden BA. The future of myopia management with contact lenses. Presented at the Global Specialty Lens Symposium, January 2015, Las Vegas.
- Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006 Dec;113:2285-2291.
- Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012 Feb;119:347-354.
- Yen M, Liu JH, Kao SC, Shiao CH. Comparison of the effect of atropine and cyclopentolate on myopia. Ann Ophthalmol. 1989 May;21:180-182,187.
- Shih YF, Hsiao CK, Chen CJ, Chang CW, Hung PT, Lin LL. An intervention trial on efficacy of atropine and multi-focal glasses in controlling myopic progression. Acta Ophthalmol Scand. 2001 Jun;79:233-236.
- Yi S, Huang Y, Yu SZ, Chen XJ, Yi H, Zeng XL. Therapeutic effect of atropine 1% in children with low myopia. J AAPOS. 2015 Oct;19:426-429.
- Wang YR, Bian HL, Wang Q. Atropine 0.5% eyedrops for the treatment of children with low myopia: a randomized controlled trial. Medicine (Baltimore). 2017 Jul;96:e7371.
- Chia A, Lu QS, Tan D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology. 2016 Feb;123:391-399.
- Huang J, Wen D, Wang Q, et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology. 2016 Apr;123:697-708.
