



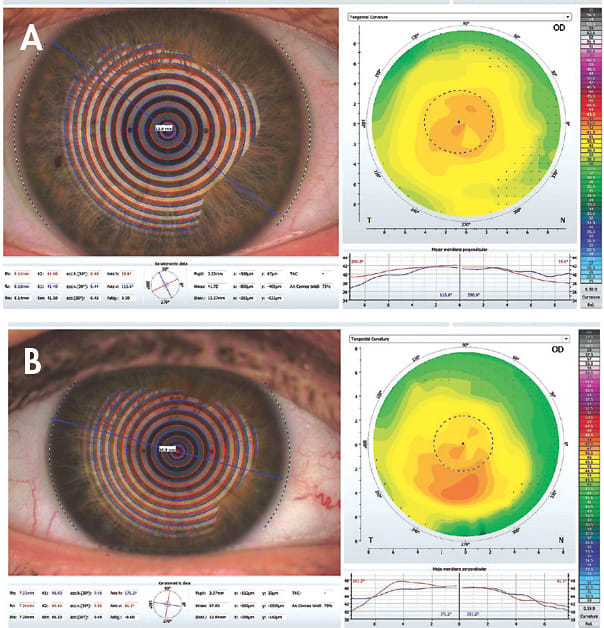
Consider two patients: both are approximately 25 years old, without notable ocular or systemic health histories. They refract to 20/20 or better in each eye with –1.00DS OD and OS in spectacles, but they struggle to find success with soft contact lenses despite trying numerous brands. Patient A complains of lens discomfort and irritation, though not necessarily dryness. Patient B complains of blur at night, with glare and great difficulty driving in the dark. Figure 1 shows their tangential corneal topography maps.
When looking to consider options beyond soft lenses, many factors should be considered and additional data taken. While many practitioners are jumping directly to more specialty (and often more expensive) lens options such as scleral, specialty soft, or hybrid lenses, it is still worth remembering the potential of a basic GP lens to provide nearly endless customizability with a very budget-friendly price tag.
From a practice management standpoint, GP lenses often include flexible warranty and return options. They also offer a lower cost to the practice if a lens is broken or lost by staff or practitioner or in those special cases in which lenses cannot be returned but customer service is more important than cost recoupment is.
Parameter Considerations
Base curve is traditionally the parameter that is considered first in GP lens fitting, but it could be argued that corneal diameter is just as important if not more so in many cases. Note the remarkable difference in both base curve and corneal diameter between patients A and B. Combining these data points into a larger perspective of sagittal depth is a worthwhile consideration. However, if this is intimidating in complexity, it is not necessary when fitting most corneal GP lenses.
Noting pupil size can be helpful when ordering or troubleshooting lenses, especially if pupil size is quite large or if multifocals are desired. Adjustments to optic zone size can be useful to aid fit and also to reduce glare complaints. It is good to note both upper and lower lid position and tension if they are abnormal in any way.
The more GP lens fitting that practitioners do, the more that these small but sometimes critical details are useful. Obtaining them at the beginning of each fit will create good fitting habits and prevent the need to troubleshoot issues later in the fitting.
Case Specifics
Patients A and B were successfully fit into GP lenses. While some adaptation was required, they were pleased with the comfort and vision that the lenses provided. The fitting process was straightforward, with lenses ordered empirically by providing critical measurements including keratometry readings, corneal diameter, pupil size, and refraction.
Patient A required a larger starting overall lens diameter than is usually suggested when corneal diameter is not provided, but he experienced surprisingly good comfort with GP lenses compared to the standard soft lens brands that were too small and steep for his corneal shape.
Patient B was fit into an aspheric GP due to the mild inferior steepening noted on topography. After a small adjustment to the optic zone, she gained a great deal in visual clarity, particularly at night, compared to her prior soft lens experiences.
While it’s still valid to approach the –1.00DS patient with soft lenses, these two seemingly simple patients had very different needs that were ultimately best met with GP lenses. With sufficient data and a good attitude from both patient and physician, GP lenses still offer exceptional value to those looking for the best in customizability and visual potential. CLS