



A 20-year-old Hispanic female presented with a history of severe bilateral dry eye and corneal scarring secondary to Stevens-Johnson syndrome (SJS) from sulfa use. The patient was fitted with a scleral contact lens in the right eye and returned for multiple follow-up visits over two years. With custom scleral devices, the patient reported symptomatic relief and improved vision, with best-corrected visual acuity (BCVA) of 20/40. Corneal changes in the right eye, including scarring, punctate epithelial erosion (PEE), and vascularization, led to a subsequent decrease in BCVA. Several ocular changes also occurred in the left eye, including a limbal stem cell transplant, corneal perforation with multiple repeat corneal transplants, cataract extraction, glaucoma tube shunt surgery, tarsorrhaphy for protection, and an eventual decline in vision. The patient was also referred for low vision services.
Ocular Complications of SJS
SJS is a severe, life-threatening mucocutaneous disease most frequently caused by an autoimmune reaction to medications or infections (Chang et al, 2007; Antoon et al, 2018; Chantaphakul et al, 2015). Toxic epidermal necrolysis (TEN) is a more severe variant of SJS that has a higher mortality rate (Antoon et al, 2018; Catt et al, 2016). The national incidences of SJS and TEN are 6.3 and 0.5 per 100,000, respectively, with a higher incidence and mortality rate in children than in adults (Antoon et al, 2018). Common causative medications include anticonvulsants, antibiotics, anti-gout agents, and non-steroidal anti-inflammatory drugs (NSAIDs) (Chang et al, 2007).
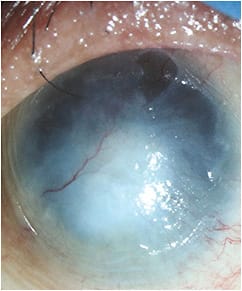
Ocular manifestations (Tables 1 and 2) occur in 60% to 88% of SJS patients, with corneal involvement in at least 18% and conjunctivitis in 78% (Chang et al, 2007; Catt et al, 2016; Chantaphakul et al, 2015). Corneal limbal stem cells are responsible for maintaining and repopulating the normal corneal epithelium when epithelial cells are shed or lost (Ahmad et al, 2010). Corneal limbal stem cell deficiency (LSCD) in the acute phase of SJS causes persistent corneal epithelial defects, conjunctivalization, recurrent corneal erosions, chronic keratitis, delayed wound healing, whorl-like epitheliopathy, vascularization (Figure 1), and loss of corneal clarity (Puangsricharern and Tseng, 1995; Chan and Holland, 2013; Kim et al, 2014).
| MILD | MODERATE | SEVERE |
|---|---|---|
| • Acute conjunctivitis • Eyelid edema • Erythema • Blepharitis • Discharge |
• Conjunctival membrane or pseudomembrane • Corneal erosion • Corneal epithelial defect |
• Cicatrizing symblepharon • Fornix foreshortening • Corneal ulcer |
| 1 DAY | Conjunctivitis, conjunctival membranes, subconjunctival hemes |
| 3 DAYS | Lid margin ulceration, corneal epithelial defects |
| 3.5 DAYS | Conjunctival ulceration |
| 4 TO 6 WEEKS | Symblepharon, trichiasis, blepharitis |
| 4 MONTHS | Chronic eyelid changes, corneal opacification (Figure 2) |
| 7 MONTHS | Limbal stem cell failure |
| 10 MONTHS | Corneal vascularization |

Treatment Options
Treatment of SJS requires hospitalization, discontinuation of causative medications, and systemic steroids and antibiotics (Chang et al, 2007; Chantaphakul et al, 2015). Ocular complications may show up months after initial presentation of SJS or hospital discharge, thus requiring life-long management, mostly due to dry eyes (Chang et al, 2007; Catt et al, 2016; Sotozono et al, 2009). Ocular manifestations of SJS may be treated with topical lubricants and topical and/or systemic steroids and antibiotics. Surgery may be needed to correct ocular structural defects and deformities (Chang et al, 2007; Chantaphakul et al, 2015; Sotozono et al, 2009).
Conservative treatments for LSCD include frequent use of preservative-free artificial tears, vitamin A ointment q.h.s., topical steroids, oral doxycycline 100mg, punctal plugs, and topical cyclosporine 0.05% (Chan and Holland, 2013; Kim et al, 2014). Limbal stem cell transplantation with systemic immunosuppression is more successful for total symptom resolution, improved vision, and ocular surface stability (Ahmad et al, 2010; Chan and Holland, 2013).
Scleral lenses may significantly improve visual acuity and function in patients who have chronic ocular manifestations of SJS (Heur et al, 2014) by stabilizing the ocular surface and reducing symptoms (Kim et al, 2014).
Conclusion
SJS is a severe disease with multiple ocular complications, including LSCD. Early treatment is important, but life-long management of both conditions may be necessary. Scleral contact lenses may improve vision and comfort in patients who have LSCD. CLS
For references, please visit www.clspectrum.com/references and click on document #283.