



Our patient is a 62-year-old female who had a history of herpes zoster (HZV) keratitis in the left eye in 2016. She was referred to our specialty contact lens clinic for possible optical management of her irregular astigmatism.
HZV is a viral infection secondary to a reactivation of the chickenpox virus that has remained dormant within a patient for many years. Herpes zoster ophthalmicus (HZO) usually occurs in individuals over the age of 50 and begins with a severe, unilateral, disabling neuralgia in the region of distribution of the ophthalmic division of the trigeminal nerve. It is followed by a vesicular eruption of the skin of the forehead, nose, eyelids, and sometimes the cornea. Ocular complications occur in approximately 50% of HZV cases and can include epithelial keratitis, with a haze and loss of stromal tissue, resulting in irregular astigmatism in the area of the central or paracentral cornea.
This patient’s right eye visual acuity was 20/25 without correction and was 20/20 with a manifest refraction of +0.50 –0.25 x 150. The uncorrected visual acuity of the left eye was 20/200; it was corrected to 20/40– with +4.50 –1.75 x 078.
Slit lamp examination was unremarkable for the right eye, and the left eye showed a faint 3.0mm diffuse central scar slightly inferior to the geometric center of the cornea. Additionally, there was a 3.5mm horizontal pigmented line just below the pupillary margin.
This form of unilateral, irregular astigmatism could be corrected with a wide range of contact lens modalities that include a GP corneal or scleral lens design, a hybrid lens, or piggyback lenses.
Our primary lens design for correcting patients who have irregular corneal astigmatism post-HZV or post-herpes simplex is a corneal GP lens. In this group of patients, corneal lenses often provide a visual acuity correction that is superior to that of scleral lenses, and they create the least amount of physiologic disruption to the cornea to lessen the chances of reactivation of the virus.
In addition, recent reports (Caroline and André, 2017; Caroline and André, 2019) have documented intraocular pressure (IOP) changes in patients wearing scleral lenses, which suggests that corneal contact lenses should be used when appropriate and that scleral lenses be used only when necessary.
Finding the Right Lens
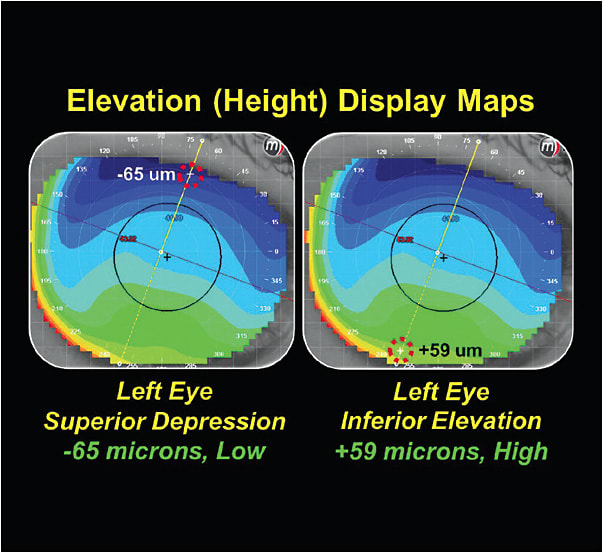
To determine whether our patient was a candidate for a corneal contact lens, we used the elevation display map to determine the height differential across the cornea. In this case, the height differential was 124 microns due to a superior depression of –65 microns and an inferior elevation of +59 microns (Figure 1). Previous studies at Pacific University (Caroline and André, 2015) have shown a high degree of fitting/wearing success with corneal contact lens designs when fitting patients who have 350 microns or less of height differential across the cornea.
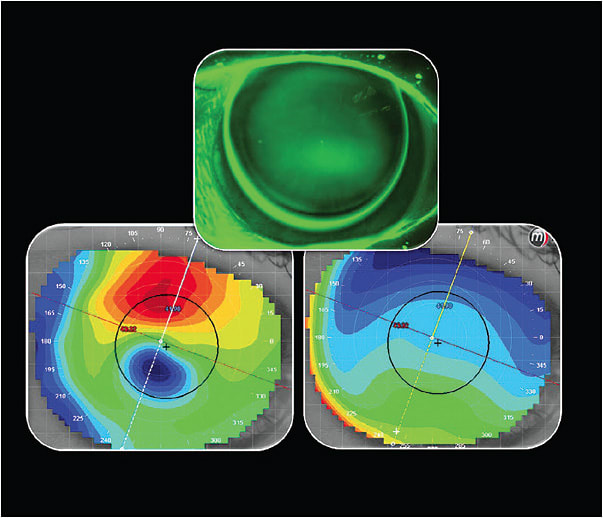
The patient’s left eye was ultimately fitted with a corneal lens design with a base curve of 43.00mm (7.75D), power +2.25, diameter 10mm (Figure 2), and she achieved 20/20-1 visual acuity and comfortable all-day lens wear. CLS
For references, please visit www.clspectrum.com/references and click on document #288.