



Modern frequent replacement soft contact lenses (CLs) are available in a wide choice of designs, materials, and replacement frequencies. Soft lens fitting data from 33 countries in 2018 showed that, on average, silicone hydrogel (SiHy) was the material of choice three-quarters of the time (76%), and for modality, daily disposables accounted for 32% of fits.1 Given the choice of CLs available, the question remains: How are these fitting decisions reached?
During a CL fit, an eyecare practitioner must navigate through all available options to reach one final recommendation that is tailored for that individual patient. That final recommendation should be based on the clinical information collected along with personal attributes of the individual patient such as hygiene habits, tobacco use, desire to sleep in his or her lenses, occupation, etc. Soft contact lenses are not “one-size-fits-all”; they are medical devices that require skill and knowledge to successfully fit. Sometimes, the initial recommendation may be driven by a patient’s request for a particular modality. The refraction may also dictate a certain material or design based on either oxygen transmissibility or prescription availability.
However, in general, the most appropriate choice for a patient is not always entirely clear. This is particularly true when fitting patients with CLs for the first time. The initial examination during CL fittings affords the opportunity to collect information about patients and also to perform baseline clinical measures of the anterior eye. This article reviews the available evidence for how this information can be used to inform the initial CL recommendation in a neophyte. In other words: Can baseline information help determine with which particular CL material or replacement frequency a patient is most likely to succeed?
PATIENT AND CLINICAL INFORMATION
Initial discussions can help to establish patients’ motivation to wear CLs, desired wearing times, and, in some cases, preferred modality. However, patients very often may not be aware of the latest clinical information or available options; hence, the importance of clinicians to educate their patients.
Corneal Infiltrative Events Beyond this information, a number of additional factors should be established to help inform the CL recommendation (Table 1). The evidence base has a recurring theme with regard to corneal infiltrative events (CIEs). These can range in severity on a spectrum from asymptomatic through to microbial keratitis (MK). A history of ocular surface disease or previous CIEs,2,3 some chronic health conditions,2 poor hygiene and the associated increased bacterial bioburden on lenses,4 smoking,3,4 and dusty environments2,5 can all elevate the risk of CIEs or MK. Should patients present with any of these risk factors, the recommendation of daily disposable CLs, a modality associated with a lower risk of CIEs, would be prudent.6
| FACTOR | EVIDENCE | CL RECOMMENDATION |
|---|---|---|
| Health and medications | ↑ CIE rate with some chronic conditions2 and smoking3,4 | Consider daily disposable |
| Seasonal allergy | ↑ Comfort26 and ↓ symptoms27 with hydrogel daily disposable | Consider hydrogel daily disposable |
| Ocular history | ↑ CIE risk if there is a history of ocular surface disease or previous CIEs2,3 | Consider daily disposable |
| Hygiene | CIEs associated with substantial bioburden on lenses4 | Consider daily disposable |
| Wearing environment | ↑ CIE risk with certain environments: dust, wind, fumes, or water2,5 | Consider daily disposable |
| Baseline symptoms (verbal), # reported on average | Tolerant: 1; Intolerant: 3 Common symptoms: dryness, foreign body sensation, stinging9 |
Combine result with tear assessment (Table 2) to better predict future success of CL wear |
| Baseline symptoms (OSDI) | Asymptomatic: 3.97 to 7.6; Symptomatic: 12.2 to 14.48*7,8 | Combine result with tear assessment (Table 2) to better predict future success of CL wear |
| * Range from two studies | ||
Baseline Symptoms A number of studies have examined whether baseline symptomology can help predict how successful a patient will be with CLs. All of those studies recommend capturing information about how the eyes feel prior to fitting CLs. This baseline symptomology can be established in several ways.
The Ocular Surface Disease Index (OSDI) is a questionnaire designed to capture symptoms associated with dry eye. When applied to prospective CL wearers, differences are evident between those subjects who, in terms of comfort, end up being either successful or unsuccessful wearers (Table 1).7,8 A modified McMonnies dry eye questionnaire that captured descriptive symptoms such as dryness, foreign body sensation, and stinging also showed differences in the average number of symptoms reported at baseline by tolerant and intolerant CL wearers (Table 1).9 In all of these studies, the ability to predict the likely future response of patients to CL wear was improved when baseline symptomology was combined with further clinical measures.
Despite the fact that symptomology does not directly inform the decision of what CL material or replacement frequency to select, establishing this information at the CL fit still has value. An informed eyecare practitioner can make use of the information to better communicate with and advise patients on their likely success with lenses and whether a modified wear schedule may be required. If baseline symptoms suggest potential future compromised CL wear, then counselling patients on the need for certain material technologies and achievable wearing times can help to set realistic expectations. Symptomology questionnaires can also help direct clinicians as to when specific clinical diagnostic testing is warranted.
Clinical Information Various clinical assessments may also assist practitioners with an initial lens selection for neophyte patients. These include evaluation of the tear film, the ocular surface, and the eyelids as detailed in the following sections.
THE IMPORTANCE OF THE TEAR FILM
Given that a number of the clinical assessments conducted when fitting CLs relate to the tear film, it is perhaps useful to recognize why so much attention falls on the tear layer. In the human eye, the typical volume of tears present on the anterior eye is 7μl,10 with a thickness over the central cornea of 3μm to 5μm.11,12 Within this small volume exists a highly complex fluid consisting of blended phases of lipid, aqueous, and mucin. The tear film performs a number of critical roles. It provides a smooth refractive surface and maintains ocular surface health and comfort. In fact, loss of tear film homeostasis has been identified as a key factor in dry eye disease.13
The addition of a CL creates a particular challenge for the tear film. The typical soft lens is many times thicker compared to the tear film, which naturally disrupts the intricate structure of the lipid, aqueous, and mucin phases; hence, it is important to establish the quality and quantity of the tear film prior to CL fitting.
TEAR ASSESSMENT TECHNIQUES
Tear Film Stability—Fluorescein Breakup Time Perhaps the most commonly conducted assessment of the tear film is fluorescein breakup time (FBUT). In this assessment, a drop of fluorescein is introduced to the tears, and the tear film is viewed with the slit lamp using blue light and a yellow barrier filter (Wratten #12). The amount of time from the last blink to the first breakup of the fluorescent tear layer is recorded. The measurement is variable, so to attain a more truly representative value, three measurements are typically averaged. This is clearly an invasive technique, with the drop of fluorescein adding between two to four times the volume of the tear film itself.14 Despite this, it is an easy technique to conduct in practice, and its value in CL recommendation has been investigated. This measure was found to provide no information on patient suitability from either a material or a modality point of view.15 There were some differences for average FBUT between successful wearers and dropouts (Table 2); however, discrimination between these values was poor.8
| FACTOR | EVIDENCE | CL RECOMMENDATION |
|---|---|---|
| TEAR STABILITY | Combine result with baseline symptoms (Table 1) to better predict future success of CL wear | |
| FBUT, seconds | Successful: 10.7 ± 6.4; Dropouts: 7.5 ± 4.78 | |
| NITBUT, seconds | Successful: 17.0 to 22.7*; Dropouts: 12.0 to 14.9*7-9 | |
| TEAR VOLUME | Combine result with NITBUT and baseline symptoms (Table 1) to better predict future success of CL wear | |
| Phenol red thread, mm | Tolerant: 16.4 ± 3.2; Intolerant: 11.9 ± 4.29 | |
| Tear meniscus height, mm | Tolerant: 0.43 ± 0.1; Intolerant: 0.31 ± 0.19 | |
| LIPCOFs | Combine result with NITBUT and baseline symptoms (Table 1) to better predict future success of CL wear | |
| LIPCOF sum (nasal & temporal grade) | Asymptomatic: 0.0 (0.00 to 1.0); Symptomatic: 2.0 (1.0 to 3.0)7 |
|
| LIDS | Consider hydrogel daily disposable | |
| Tarsal conjunctiva | ↑ comfort26 and ↓ symptoms27 with hydrogel daily disposable | |
| Blepharitis and meibomian gland dysfunction | ↓ CIE risk resulting from ↑ Gram-positive bacteria by using daily disposable | Consider hydrogel daily disposable |
| * Range from three studies | ||
Tear Film Stability—Non-Invasive Breakup Time Tear stability can be assessed using non-invasive methods, which would typically be conducted early in the examination. Common to all non-invasive tear breakup-time (NITBUT) techniques is the principle of shining an image, such as a Placido disc, onto the tear film and determining when the projected image distorts as the tear film breaks up post-blink. An average of three measurements is typically calculated. Some care is necessary when interpreting NITBUT results, as average quoted times for breakup can vary depending on whether a “blur” or a “break” in the image has been used as the endpoint.
A number of studies have examined whether the NITBUT recorded at baseline in a neophyte corresponds to future CL wear. The average NITBUT was significantly higher in each study for those termed either “successful” or “tolerant” CL wearers compared to those who were not (Table 2).7-9
However, NITBUT does not provide useful information with regard to material or modality, with a recent study confirming that the final choice of silicone hydrogel or hydrogel material after four hours of wear was based on visual acuity, fit, and comfort and did not correlate with tear film surface quality.16
Tear Volume In addition to measures of tear film stability, an assessment of tear volume should be conducted to more completely describe the tear film. Invasive methods such as the Schirmer’s test and the phenol red thread test quantify the amount of tears produced in a set amount of time. Significantly lower tear volume has been recorded for intolerant CL wearers using the phenol red thread test, with the study concluding that CL intolerance is best predicted by combining the results of baseline symptoms, tear stability, and tear volume.9
The height of the tear meniscus along the lower lid can also be measured to provide a non-invasive estimate of tear volume. Again, intolerant CL wearers have significantly lower values;9 however, discrimination between groups based on this measure alone is difficult.
Osmolarity The recent Tear Film & Ocular Surface Society Dry Eye Workshop (DEWS) II report highlights that tear film hyperosmolarity is a key part of the mechanism of dry eye.13 For CLs, however, the evidence is equivocal, with debate as to whether lens type and wear modality affect osmolarity in CL wearers and whether this ultimately influences CL comfort. One study reported higher osmolarity in patients who have CL-related dryness,17 but another could not find an association between tear osmolarity and ocular comfort during CL wear.18 A recent study reported no significant difference in tear film osmolarity and other ocular surface measures after wear of either hydrogel or SiHy lenses.19 With the increasing availability in practice of instruments that can measure this parameter, research that helps further our understanding of the relevance of tear film osmolarity to successful CL wear, particularly as to whether it can inform about appropriate material or modality, would be welcome.
Lipid Layer Assessment The tear lipid layer plays a role in preventing evaporation of the tear film. Interferometry allows the flow of lipid over the surface of the tear layer to be visualized and the thickness of the layer to be estimated. CL wear impairs tear film lipid layer integrity and spread, and this has been correlated with CL discomfort.20 While lipid layer thickness is quoted to be 50nm to 100nm,21 it is not currently clear how—or whether—baseline lipid layer thickness correlates to the success of future CL wear.
In addition to the lack of information with regard to lipid layer thickness, the quality of the lipid layer is another unknown consideration. Similar to measures of osmolarity, this is another area in which more information would be welcome and in which current evidence does not inform CL material or modality choice.
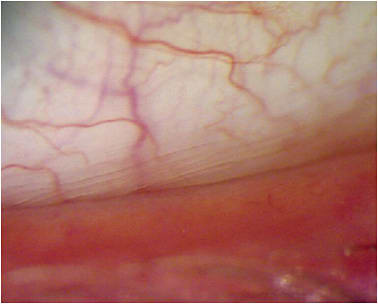
LID PARALLEL CONJUNCTIVAL FOLDS
Thought to be related to ocular dryness, lid parallel conjunctival folds (LIPCOFs) can be viewed and graded along the nasal and temporal inferior lid margins (Figure 1). While not informing the choice of CL material or replacement frequency, LIPCOF grade is often significantly higher in symptomatic compared to asymptomatic CL wearers (Table 2).7 The same study also concluded that the best prediction of dry eye symptoms developing in CL wearers resulted from combining the findings of the OSDI questionnaire, NITBUT, and LIPCOFs.7
OCULAR SURFACE ASSESSMENT
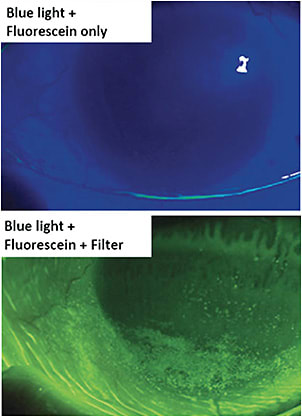
Several elements of the biomicroscope examination need to be conducted during a CL fitting regardless of whether the results can inform the CL recommendation. These are primarily anterior eye health and safety evaluations and may include assessment of bulbar and limbal hyperemia, assessment of the function and structure of the meibomian glands, a detailed view of the cornea, and checking the integrity of ocular surface tissues with sodium fluorescein. With regard to corneal staining, the evidence remains too equivocal to link its presence to CL discomfort.22 Remember that the best view of fluorescein staining is achieved by using cobalt blue illumination with a yellow barrier filter (Figure 2).
LID ASSESSMENT
When assessing the lids, establish the baseline appearance of the tarsal conjunctiva and lid margins. Also check for the presence of pathology such as blepharitis and meibomian gland dysfunction (MGD). Given the more invasive nature of some lid assessment techniques, such as lid eversion and meibum expression, it is sensible to reserve these assessments for near the end of the anterior eye examination.
Inexpensive devices are available that allow clinicians to apply consistent pressure to the lid margin in a minimally invasive manner to facilitate grading of meibomian gland function. A variety of imaging technologies are also now being used in clinical practice to provide morphological information on the structure of the meibomian glands.23-25
In contrast to the many tear film measures, which at best may predict whether CL wear will be symptomatic or not, a number of lid-related findings can inform the initial CL recommendation. Evidence of tarsal conjunctival inflammation in the form of hyperemia and papillae, particularly when accompanied by a reported history of seasonal allergy, can indicate the recommendation of daily disposable CLs. While all daily disposable options will minimize the buildup of deposits and allergens, the current evidence specifically reports on the protective effect and increased comfort achievable with hydrogel daily disposables.26,27
Compared to healthy lid margins, those with blepharitis28,29 or MGD30 are associated with a higher presence of Gram-positive bacteria such as Staphylococcus aureus; high levels of Gram-positive microorganisms are associated with CIEs in the form of marginal keratitis, which typically presents where the lid margins touch the cornea at 2 o’clock, 4 o’clock, 8 o’clock, and 10 o’clock. In addition to standard treatment and long-term management measures, this sequelae can be minimized and the risk of CIEs can be lowered by recommending daily disposable CLs.31,32 MGD is now recognized as the major cause of dry eye, with up to 86% of dry eye patients exhibiting signs of MGD.33 Thus, it is important to identify this condition early and to address it with a targeted approach if comfortable CL wear is to be achieved.
Demodex mites live in human sebaceous glands and hair follicles. When present in eyelash follicles, they form distinctive collarettes around the base of the lashes (Figure 3), and treatment to remove the debris and resolve the infestation is recommended. Their presence is relevant to CL wear, with a higher proportion of CL wearers positive for Demodex and with a significantly higher number of mites per subject than in non-CL wearers (7.6 versus 5.0; p = 0.02).34 In a further study, the presence of Demodex was also associated with CL dropout, with 93% of dropouts having mites compared to 6% of asymptomatic wearers.35 While not helping in terms of the CL recommendation, this evidence does highlight the importance of looking for and treating Demodex infestation in prospective and current CL wearers.

CONCLUSIONS
Clinicians collect a large amount of information when fitting patients with CLs, both in terms of history, symptoms, and lifestyle and in terms of many baseline measures of the anterior eye. A review of the current evidence base demonstrates that some of this information can be used to help with recommendation of a specific CL material or replacement frequency. This is most often true with information established via patient history and through careful review of the eyelids.
In many situations, however, what is measured and recorded does not directly inform our CL recommendation. The tear film is a prime example; clinicians understand its importance and have the ability to assess it in a number of ways, yet they cannot use that information to select a specific CL. The best available evidence right now suggests that we can predict whether a patient will likely be symptomatic or asymptomatic in CLs by combining the results of baseline symptoms, NITBUT, and either tear meniscus height or LIPCOFs. New technologies that allow clinicians to gauge the function and structure of the meibomian glands provide the knowledge and information to introduce treatments to optimize the ocular surface. It is clear upon a review of the literature that truly tailoring the soft CL recommendation to each patient’s own individual tear film is an area that requires significant further research. CLS
Editorial support for this article provided by Gabriella Courey, OD; MSc Candidate – Cornea and Contact Lens, École d’optométrie, Université de Montréal.
REFERENCES
- Morgan PB, Woods CA, Tranoudis IG, et al. International Contact Lens Prescribing in 2018. Contact Lens Spectrum. 2019 Feb;34:26-32.
- Keay L, Edwards K, Stapleton F. Signs, symptoms, and comorbidities in contact lens-related microbial keratitis. Optom Vis Sci. 2009 Jul;86:803-809.
- McNally JJ, Chalmers RL, McKenney CD, et al. Risk factors for corneal infiltrative events with 30-night continuous wear of silicone hydrogel lenses. Eye Contact Lens. 2003;29:S153-S156; discussion S66, S92-S94.
- Szczotka-Flynn L, Lass JH, Sethi A, et al. Risk factors for corneal infiltrative events during continuous wear of silicone hydrogel contact lenses. Invest Ophthalmol Vis Sci. 2010 Nov; 51:5421-5430.
- Ozkan J, Mandathara P, Krishna P, et al. Risk factors for corneal inflammatory and mechanical events with extended wear silicone hydrogel contact lenses. Optom Vis Sci. 2010 Nov;87:847-853.
- Chalmers RL, Hickson-Curran SB, Keay L, et al. Rates of adverse events with hydrogel and silicone hydrogel daily disposable lenses in a large postmarket surveillance registry: The TEMPO Registry. Invest Ophthalmol Vis Sci. 2015 Jan 8;56:654-663.
- Pult H, Murphy PJ, Purslow C. A novel method to predict the dry eye symptoms in new contact lens wearers. Optom Vis Sci. 2009 Sep;86:E1042-E1050.
- Best N, Drury L, Wolffsohn JS. Predicting success with silicone-hydrogel contact lenses in new wearers. Cont Lens Anterior Eye. 2013 Oct;36:232-237.
- Glasson MJ, Stapleton F, Keay L, et al. Differences in clinical parameters and tear film of tolerant and intolerant contact lens wearers. Invest Ophthalmol Vis Sci. 2003 Dec;44:5116-5124.
- Mishima S, Gasset A, Klyce SD Jr., et al. Determination of tear volume and tear flow. Invest Ophthalmol Vis Sci. 1966 Jun;5:264-276.
- Wang J, Fonn D, Simpson TL, et al. Precorneal and pre- and postlens tear film thickness measured indirectly with optical coherence tomography. Invest Ophthalmol Vis Sci. 2003 Jun;44:2524-2528.
- King-Smith PE, Fink BA, Hill RM, et al. The thickness of the tear film. Curr Eye Res. 2004 Oct-Nov;29:357-368.
- Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017 Jul;15:276-283.
- Mooi JK, Wang MTM, Lim J, et al. Minimising instilled volume reduces the impact of fluorescein on clinical measurements of tear film stability. Cont Lens Anterior Eye. 2017 Jun;40:170-174.
- Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017 Jul;15:539-574.
- Mousavi M, Jesus DA, Garaszczuk IK, et al. The utility of measuring tear film break-up time for prescribing contact lenses. Cont Lens Anterior Eye. 2018 Feb;41:105-109.
- Nichols JJ, Sinnott LT. Tear film, contact lens, and patient-related factors associated with contact lens-related dry eye. Invest Ophthalmol Vis Sci. 2006 Apr;47:1319-1328.
- Stahl U, Willcox MD, Naduvilath T, et al. Influence of tear film and contact lens osmolality on ocular comfort in contact lens wear. Optom Vis Sci. 2009 Jul;86:857-867.
- Ruiz-Alcocer J, Monsalvez-Romin D, Garcia-Lazaro S, et al. Impact of contact lens material and design on the ocular surface. Clin Exp Optom. 2018 Mar;101:188-192.
- Craig JP, Willcox MD, Argueso P, et al. The TFOS International Workshop on Contact Lens Discomfort: Report of the Contact Lens Interactions With the Tear Film Subcommittee. Invest Ophthalmol Vis Sci. 2013 Oct 18;54:TFOS123-TFOS156.
- King-Smith PE, Hinel EA, Nichols JJ. Application of a novel interferometric method to investigate the relation between lipid layer thickness and tear film thinning. Invest Ophthalmol Vis Sci. 2010 May;51:2418-2423.
- Efron N, Jones L, Bron AJ, et al. The TFOS International Workshop on Contact Lens Discomfort: Report of the Contact Lens Interactions With the Ocular Surface and Adnexa Subcommittee. Invest Ophthalmol Vis Sci. 2013 Oct 18;54:TFOS98-TFOS122.
- Pult H, Nichols JJ. A review of meibography. Optom Vis Sci. 2012 May;89:E760-E769.
- Arita R, Itoh K, Maeda S, et al. A newly developed noninvasive and mobile pen-shaped meibography system. Cornea. 2013 Mar;32:242-247.
- Ngo W, Srinivasan S, Schulze M, et al. Repeatability of grading meibomian gland dropout using two infrared systems. Optom Vis Sci. 2014 Jun;91:658-667.
- Hayes VY, Schnider CM, Veys J. An evaluation of 1-day disposable contact lens wear in a population of allergy sufferers. Cont Lens Anterior Eye. 2003 Jun;26:85-93.
- Wolffsohn JS, Emberlin JC. Role of contact lenses in relieving ocular allergy. Cont Lens Anterior Eye. 2011 Aug;34:169-172.
- Lindsley K, Matsumura S, Hatef E, et al. Interventions for chronic blepharitis. Cochrane Database Syst Rev. 2012 May 16:CD005556.
- Teweldemedhin M, Gebreyesus H, Atsbaha AH, et al. Bacterial profile of ocular infections: a systematic review. BMC Ophthalmol. 2017 Nov 25;17:212.
- Watters GA, Turnbull PR, Swift S, et al. Ocular surface microbiome in meibomian gland dysfunction. Clin Exp Ophthalmol. 2017 Mar;45:105-111.
- Chalmers RL, Keay L, McNally J, et al. Multicenter case-control study of the role of lens materials and care products on the development of corneal infiltrates. Optom Vis Sci. 2012 Mar;89:316-325.
- Steele KR, Szczotka-Flynn L. Epidemiology of contact lens-induced infiltrates: an updated review. Clin Exp Optom. 2017 Sep;100:473-481.
- Lemp MA, Crews LA, Bron AJ, et al. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012 May;31:472-478.
- Jalbert I, Rejab S. Increased numbers of Demodex in contact lens wearers. Optom Vis Sci. 2015 Jun;92:671-678.
- Tarkowski W, Moneta-Wielgos J, Mlocicki D. Demodex sp. as a Potential Cause of the Abandonment of Soft Contact Lenses by Their Existing Users. Biomed Res Int. 2015;2015:259109.