



The benefits of providing unaided myopia correction during waking hours through the use of orthokeratology (OK) contact lens wear is well known. OK’s popularity is growing, as evidence shows a reduction in pediatric myopia progression by around half in two-year meta-analyses (Sun et al, 2015; Si et al, 2015). Additionally, a recent survey indicated that 52% of myopia control contact lens fits to children are OK (Efron et al, 2019). While this paints a positive picture of proactive myopia control contact lens fitting, only 2.3% of contact lens fits to children are for this purpose (Efron et al, 2019), which indicates a professional reticence to embrace OK and multifocal soft contact lenses (MFCLs) for their benefits of both myopia control and correction.
Levels of Understanding
I’d like to address some key differences between OK and MFCLs in pediatric myopes, levelling up from understanding the “add” of each through to optical and binocular vision alterations. Note: I will use MFCL for any type of multifocal or dual-focus soft contact lens that has been investigated for myopia control unless specified otherwise.
Level 1: How do the adds compare? Various designs of MFCLs have been evaluated for myopia control efficacy, showing results of around 30% to 50% control for both refractive and axial length change on meta-analysis (Li et al, 2017). There is a belief that a higher add in a MFCL will create a greater shift in relative peripheral refraction and therefore a better myopia control effect, but this has yet to be proven beyond anecdotal accounts. The basis for this is likely that MFCLs are less predictable in their induced peripheral refraction shift compared to OK (Ticak and Walline, 2013). OK generates a myopic shift in relative peripheral refraction in a 1:1 relationship to the central refractive change (Queirós et al, 2010; Kang and Swarbrick, 2010). By comparison, a study evaluating a +2.00D add distance-centered MFCL for myopes of –2.8D on average reported no significant shift from the baseline peripheral refractive profile compared to the predictable shift generated from OK wear (Ticak and Walline, 2013). An industry project in which a MFCL was designed to “mimic OK” in its anterior optical profile was recently reported as having no significant benefit for myopia control, indicating that MFCLs and OK present different optical properties to the eye (Cheng et al, 2018). The authors postulated a possible mechanical mechanism for OK, but the peripheral refractive shift of the novel MFCL was not confirmed to match that of OK in a similar power.
The Bifocal Lenses in Nearsighted Kids (BLINK) multi-site study is currently investigating distance-centered MFCLs with a +1.50D and +2.50D add to evaluate differences in myopia control efficacy and peripheral refractive shift (Walline et al, 2017). When available, these results will greatly assist our understanding of how the add influences the myopia control effect and could cross-transfer to improved understanding in OK. There is still a way to go before we are able to define which lens type is best based on patients’ level of myopia, excepting for myopia greater than 4D to 5D in which OK treatment becomes more challenging, dependent on corneal shape (Mountford, 1997).
Level 2: Do smaller OK treatment zones provide better myopia control? OK treatment generally results in a 4mm to 6mm central zone of topographical flattening to correct myopia (Tahhan et al, 2003), while a much smaller central optic zone in MFCLs reduces acuity and can require myopic over-correction. (Schulle et al, 2018). Some believe that reducing the treatment zone diameter (TZD) with an OK lens will increase the relative peripheral myopic shift achieved and, therefore, lead to a better myopia control effect.
This assumption is likely based on a study in which there was a better myopia control effect in subjects who had larger pupil diameters compared to those who had smaller pupils; a scotopic diameter of 6.4mm was the average and the delineation point (Chen et al, 2012). The authors speculated that larger pupils allowed for a greater peripheral surface area of defocus, but peripheral refractive shift was not measured.
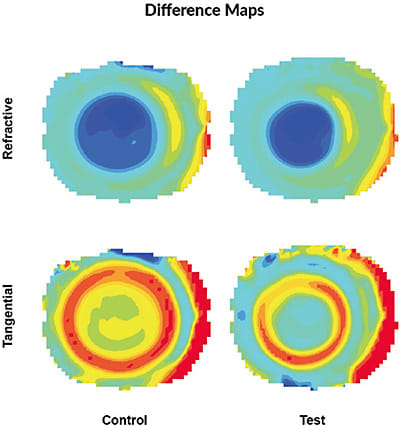
Anecdotal reports of better myopia control with OK lenses designed to produce a smaller TZD are not new, but evidence showing that such lenses actually result in an altered topographical outcome is quite new (Marcotte-Collard et al, 2018). Since then, further research has shown that successfully reducing the TZD from 6mm to 5mm (Figure 1) did not result in a change in relative peripheral refraction as postulated (Gifford, Kang, et al, 2019). If the anecdotal reports of small TZDs providing better myopia control efficacy are to believed, this might indicate that relative peripheral refraction is not the driving mechanism.
Level 3: How could OK control myopia if it’s not via peripheral refraction? The other key optical change resulting from altering corneal topography with OK is higher-order aberrations (HOAs). OK dramatically increases HOAs (Stillitano et al, 2008), and key HOAs such as spherical aberration and coma have been correlated to the myopia control effect (Hiraoka et al, 2015). Larger total corneal HOAs have even been correlated with reduced myopia progression in spectacle-corrected myopic children (Hiraoka et al, 2017).
The aforementioned work on reduced TZD in OK was further expanded upon in a study in which the smaller TZD lens increased the spherical aberration for pupil sizes of 2mm to 4mm (Gifford, Tran et al, 2019). This agrees with the clinical suggestion to fit smaller TZD OK lenses for myopia control, especially for patients who have smaller pupils; if spherical aberration is a driving mechanism, smaller pupil sizes will likely experience greater levels in these modified designs.
The flip side of this, though, is that smaller TZDs can degrade acuity when pupils become larger—Gifford, Tran, et al (2019) found that, at pupil sizes of 5mm to 7mm, the central myopic correction of OK was reduced in such a design. It is important to keep our focus on achieving good myopia correction while also controlling it.
Level 4: How does OK influence near visual function? Building on the previous level, the change in HOAs due to OK also influences the refractive state at near. After only one week of OK wear, a comparison of corneal to total eye HOAs indicates that the accommodation system adapts and increases its tone (Gifford et al, 2013), leading to reduced accommodative lags (Gifford, Gifford, et al, 2019). One Chinese study showed that lower-than-average accommodators had a 56% better myopia control effect than above-average accommodators did (defined only on their accommodative amplitude) (Zhu et al, 2014), indicating that OK may have a dual benefit for the former through both supporting near-point visual function and myopia control. By comparison, in young myopic adults, continuous aspheric MFCL designs reduce the accommodation system’s response, effectively increasing accommodative lags, whereas a concentric, dual-focus design does not influence accommodation compared to a single-vision distance soft contact lens (Gifford, Schmid, et al, 2019).
Continuous aspheric designs can also degrade near acuity more compared to a concentric design or single vision in young adult myopes (Schmid et al, 2019). Near acuity in OK wear has not been reported, but both high- and low-contrast distance acuities in high- and low-luminance conditions at distance show no degradation due to OK wear (Johnson et al, 2017).
The View From the Summit
OK provides a consistent shift in relative peripheral refraction—if this is in fact its mechanism of myopia control—and may provide better distance (Schulle et al, 2018) and near acuity than comparatively powered MFCLs can due to OK’s larger central optic zone of treatment. Reducing the central TZD of OK, which is purported to improve its myopia control effect, doesn’t appear to alter relative peripheral refraction but may instead alter ocular aberrations. This could in turn help to describe the relationship of efficacy to pupil size, although reducing the TZD could reduce the myopia correction. Finally, OK appears to support near point function by inducing an increased accommodative response in young wearers; while there is still a lot to learn, early indications are that some MFCLs may do the opposite and reduce the accommodative response, which could potentially impact their efficacy (Faria-Ribeiro et al, 2018; Cheng et al, 2019).
There’s much OK research to watch, but until we learn more, OK of any lens design can be considered a reliable option for pediatric myopia control (Sun et al, 2015). CLS
For references, please visit www.clspectrum.com/references and click on document #288.