



Contact lenses have evolved substantially over the last decade. For many practitioners, they are an important portion of the care that is provided to patients. As such, it is imperative for practitioners to pay particular attention to their contact lens practice to help patients successfully utilize this tremendous vision-correcting option. Additionally, it is critical to offer contact lenses as options for appropriate lens wearers whose ocular health, refractive error, and motivation are appropriate for contact lenses.
There are a number of competitive factors that are challenging traditional access to contact lenses. Increasing numbers of contact lens retailers are competing for our contact lens patients. Some retailers attempt to make contact lens substitutions from the specific lenses that eyecare practitioners have prescribed for their patients to lenses of the retailers’ choice. From a clinical perspective, eyecare practitioners know that there are significant differences that exist among contact lens designs, materials, and surface properties. These differences make certain lenses unwearable for some patients while others feel so comfortable that they can wear the lenses all day.
In this era of change in contact lenses, there are many challenges but also opportunities for clinicians interested in providing advanced contact lens care within their practices. But, as the industry evolves, it is critical to offer those technologies that are best suited for each individual patient. Throughout the remainder of this article, those strategies that can help take a contact lens practice to the next level will be discussed.
INCORPORATING NEW TECHNOLOGIES
There are several technologies that are available to help practitioners better diagnose and monitor corneal conditions. Additionally, technologies are now giving us greater insights into optimizing contact lens outcomes. The following is a review of some of those technologies. Although this is not a comprehensive list of technologies utilized in a contact lens practice, it provides a basis for improving fitting strategies along with increasing educational and compliance efforts for our patients.
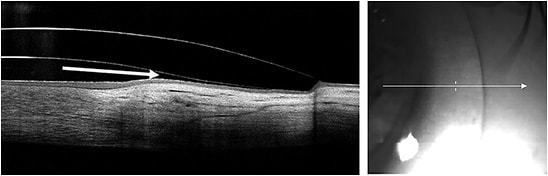
Optical Coherence Tomography (OCT) OCT has changed the way that eyecare practitioners monitor corneal conditions as well as the way that they optimize contact lens fits. For years now, scleral lens practitioners have been utilizing anterior segment OCT (AS-OCT) to measure central corneal clearance and to ensure limbal clearance. Additionally, the landing zone can be assessed utilizing AS-OCT to determine the appropriate fit (Figure 1).
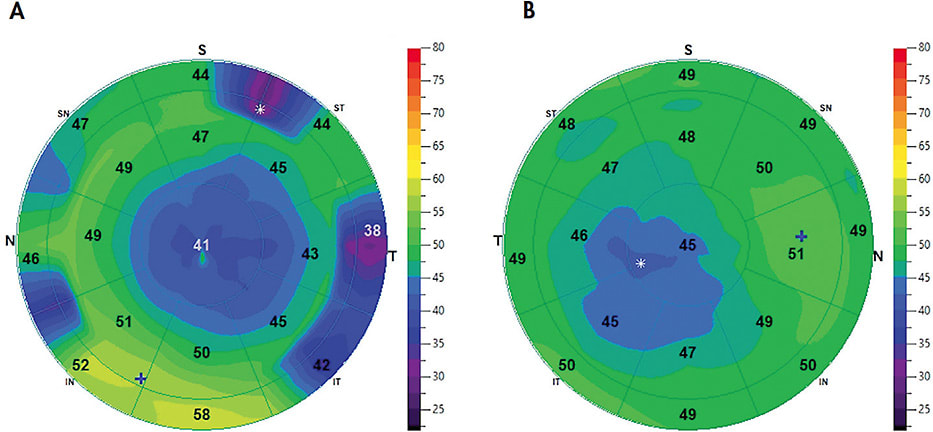
Anterior segment epithelial thickness mapping (ETM) now provides additional information on the anterior segment corneal health. Many practitioners are utilizing this in dry eye management, post-refractive surgery monitoring, and to monitor corneal dystrophies, among other purposes. Additionally, it can play a role in managing orthokeratology treatments. For example, topography measurements have traditionally been utilized to determine orthokeratology treatment centration; ETM can also now be utilized to visualize the treatment area and its centration. Ideally, this can help explain visual disruption in a seemingly normal corneal topography and can help in making appropriate changes to the lens (Figure 2).
Corneal Topography Corneal topography has been a mainstay in monitoring corneal conditions. Many practitioners have incorporated it into their comprehensive eye examination for contact lens wearers. As such, they are able to diagnose several corneal ectasias much sooner than they have been able to in the past. In doing so, they now have the opportunity to educate their patients sooner about their condition and to provide more appropriate vision correction options at an earlier stage of the disease.
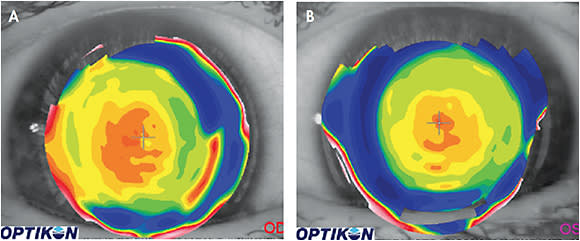
New insights into topography use have also allowed this technology to be repurposed to aid in multifocal fits. Soft multifocal contact lenses present an opportunity for presbyopes to have both distance and near vision correction. Over the last several years, practitioners have learned significantly more about the line of sight and the importance of optical alignment of a multifocal design to optimize visual outcomes.1,2 Because the multifocal optics are located on the anterior surface of a soft lens, a topographer can determine where the near and distance optics are located on the lens. Steeper curves on the anterior surface of the lens will be associated with more plus powers, which will be associated with the near optics of the lens. Distance optics will have flatter curves compared to the near optics.
Interestingly, because most topographers can also identify a patient’s line of sight, practitioners can determine where the patient’s line of sight is with respect to the optics of the multifocal lens (Figure 3). This can help explain certain multifocal failures; some patients may require a lens in which the optic zones can be re-aligned to better match with their line of sight.
Imaging Technology Anterior segment imaging has greatly advanced over the last several years. It allows clinicians to immediately capture anterior segment images of ocular surface conditions and contact lenses. This is especially important with contact lens wearers. The ease of use and convenience along with the high quality of the images produces an examination flow that is top-notch without compromising quality.
Current technologies allow practitioners to open the imaging software and to be ready to capture images with as little as three clicks of the mouse. Although this isn’t a new technology, advances in image quality—along with software updates that have optimized its utilization during examinations—have made it an exceptional tool in practitioners’ armamentarium to improve educational and compliance efforts with their patients.
OPTIMIZING NEW DESIGNS AND TECHNOLOGY
As new technologies emerge to help current contact lens wearers and to improve the experience of those new to lens wear, it is critical to embrace these technologies and to utilize them with the patients who may benefit from them.
Daily Disposable Contact Lenses Daily disposables provide a considerable advancement in convenience, comfort, and health to contact lens wearers. They are ideally suited for part-time wearers because patients will never have to worry about the age of their lenses. Additionally, there are advantages to those who choose to wear lenses on a full-time basis; these patients do not have any need for multipurpose solutions to care for their lenses, and they have the advantage of a applying new lenses to their eyes every day.
At one time, there were a limited number of options available in the daily disposable modality. Today, there are not only spheres available, but toric and multifocal lenses are available as well, all in a wide range of powers. Interestingly, this allows a large percentage of patients who have regular corneas to be candidates for daily disposable lenses. For those eligible for daily disposables, consider this option for them.
New Materials GP lenses continue to be a viable opportunity for vision correction. An increase in scleral lens fittings has made practitioners more cognizant of the importance of oxygen permeability. Recently, a new material was introduced that has a Dk of 200. This certainly is a welcome addition to increase scleral lens fitting success.
New Designs There have been several recent advancements in soft contact lenses that are noteworthy to review here. The first is the availability of a soft multifocal toric lens with fitting sets that can be stored in the office for immediate fitting of appropriate candidates. This lens is made of samfilcon A, which is a silicone hydrogel material that has a 46% water content and a Dk/t of 163. The lens has a near-center distance-periphery design that provides a specialty fit directly from the fitting set.
The second is a contact lens that darkens when exposed to ultraviolet radiation (UV). This lens is made of senofilcon A, which is a silicone hydrogel material that has a 38% water content and a Dk/t of 121. It is important to note that even though this lens does darken, it does not replace the need for sunglasses.
New Coatings A polyethylene glycol (PEG)-based coating is available that is applied to GP lenses at the laboratory. It alters the surface properties of a GP lens by increasing hydrophilic properties and also reduces deposits on the lens. This coating has been a beneficial addition in our collection of strategies to help patients wear their contact lenses more comfortably.
Make sure to educate patients regarding which solutions are appropriate to use if their lenses have the PEG-based coating on them. The lenses should never be rinsed with tap water, as it can remove the coating. The lenses should also be cleaned and disinfected only with certain hydrogen peroxide and multipurpose solution systems.
RESPECT THE OCULAR SURFACE
With all of the advancements in contact lenses, the number one reason why patients discontinue lens wear is still discomfort, with dryness being the most common symptom.3 New technologies that can help optimize surface properties of the lens may be able to partially improve dryness symptoms.4
Additionally, the ocular surface needs to be cared for to ensure comfortable contact lens wear.5 Over the last decade, there have been tremendous advances in practitioners’ understanding of the ocular surface and also of the treatments that are available to maintain and re-establish a healthy ocular surface. The Dry Eye Workshop II (DEWS II) report has provided useful guidance on both diagnosis and treatment strategies for ocular surface disease. From a diagnostic perspective, it is clear that most forms of dry eye are actually a combination or mixed etiology of both evaporative and aqueous deficient dry eye.6 This understanding helps physicians provide strategies to better diagnose and set appropriate treatment strategies for their patients who have dry eye.
With contact lens wearers, it is important to respect the health of the ocular surface and to optimize its function so that it is robust enough to support healthy lens wear. With that in mind, diagnosing any compromise to the ocular surface is critical. Each practice should have a process in place to help identify those individuals. This process can include questionnaires (Standard Patient Evaluation of Eye Dryness [SPEED], Ocular Surface Disease Index [OSDI], etc), careful assessment of the lid margin and ocular surface including vital dyes, advanced diagnostic imaging including anterior segment photography and meibography, and higher diagnostic tools including assessments such as measuring elevated levels of inflammation and tear osmolarity.
It is then incumbent upon practitioners to make clinical judgements on the major contributing factors from the diagnostic workup and to set an appropriate treatment plan to manage the ocular surface appropriately. Although this article is not a comprehensive article on managing the ocular surface, here are a few clinical pearls on how to manage those components that can contribute to uncomfortable lens wear.
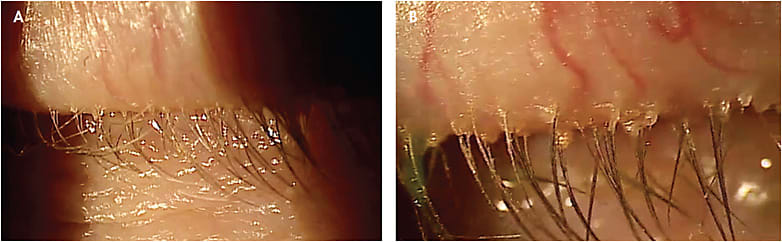
Manage the Lid Margin It is necessary to optimize the health of the lids. Pay particularly close attention to the base of the lashes for signs of inflammation and also for deposits at the base of the lashes that can contribute to signs and symptoms of dry eye (Figure 4).7 Microblepharoexfoliation is an in-office procedure that exfoliates the lid margin and reduces its bacterial bioload.
Ongoing lid health habits are vital for these individuals to ensure that they maintain the health of the lids and to keep bacterial populations at low levels. Hypochlorous acid is an effective and gentle way to maintain lid margin health. If Demodex overpopulation is suspected, a lid maintenance routine that includes high-concentration tea tree oil is recommended.8,9
Included in appropriate lid margin management is optimizing the function of the meibomian glands. Currently, three procedures to optimize meibomian gland function are available to perform in-office:
- In one procedure, the meibomian glands are heated from the posterior surface of the lid while there is a simultaneous inflatable bladder that repeatedly applies pressure to the anterior surface of the lid. This is a closed-eye procedure. A single treatment has been shown to increase comfortable lens wear by four hours.10
- In a second procedure, the meibomian glands are heated from the posterior surface of the lid, and clinicians apply pressure to the anterior lid margin while viewing the expression of meibum from the gland orifices.
- In a third procedure, a pad-like device is applied to the anterior surface of the lids that applies heat to the lids for 15 minutes. Meibum from the glands is then expressed at the slit lamp using an expressor paddle.
Reducing Inflammation It has long been known that dry eye is an inflammatory condition. There are several ways to reduce inflammation on the ocular surface:
- Topical Corticosteroids Topical corticosteroids reduce inflammation on the ocular surface. These are typically used for a short duration to avoid the potential ocular side effects that can result from long-term corticosteroid use. Often, clinicians will pulse corticosteroids for dry eye flare ups and then discontinue use when the inflammation subsides.
- Ocular Nutrition Several nutrients can reduce inflammation on the ocular surface. Specifically, high doses of quality omega-3 essential fatty acids have been shown to reduce inflammatory levels of cytokines on the surface of the eye and to improve contact lens comfort.11
- Cyclosporine This has been commercially available at 0.05% for some time. It also recently launched in the United States at a 0.09% concentration. Cyclosporine reduces inflammation through T-cell modulation. Contact lens wearers randomized to either placebo (carboxymethylcellulose 0.5% rewetting drops) or 0.05% cyclosporine demonstrated improvement in contact lens comfort after five weeks with the use of 0.05% cyclosporine.12
- Lifitegrast This is commercially available at 5%. It is a lymphocyte function associated antigen-1 (LFA-1) antagonist. This prevents LFA-1 on T-cells from interacting with intercellular adhesion molecule-1 (ICAM-1), which is over-expressed on the inflamed ocular surface. In a single-center, prospective, open-label study, contact lens wearers showed improved contact lens symptoms after eight weeks of lifitegrast dosed twice a day.13
Tear Retention In the absence of lid margin disease and when inflammation is controlled, punctal plugs may benefit those who have contact lens discomfort. There are silicone plugs that are visible at the puncta when inserted and intracanalicular plugs. In a small study of symptomatic lens wearers, silicone plugs were placed in the lower punctum of one eye, with no plug placed in the other eye’s punctum.14 Most study subjects experienced significant improvements in comfort in the eye that was occluded when the silicone plugs were used.14
MANAGE MYOPIA
Traditionally, myopia has been managed by correcting a patient’s refractive error. Unfortunately, from a clinical perspective, correcting just the refractive error does not provide the means to control the rate of myopia progression. Over the last decade, researchers and practitioners have gained significant insights into not only correcting the refractive error of progressing myopes but also managing the disease by slowing the rate of myopia progression. Globally, the prevalence of myopia is 28.3% and is expected to increase to 49.8% by 2050.15 Although myopia management can involve spectacle lenses and/or atropine as well, here is a review of those contact lens options that help manage myopia progression. Note that contact lenses to slow progression of myopia is still an off-label use in the United States.
Orthokeratology This involves the remolding of the cornea to flatten its central area to correct myopic refractive error. Interestingly, this creates a reverse curve in peripheral portions of the cornea that generates peripheral myopic defocus. This is what seems to alter the trajectory of myopia progression and to slow the rate of progression.16,17
Long-term safety and efficacy have been well established with overnight orthokeratology use for the management of myopia.18,19 In a recent review of several studies, orthokeratology demonstrated a positive effect on myopia progression by reducing its progression by 45% as measured by axial length.20 Orthokeratology is a viable option for managing myopia and is an important option to embrace for appropriate candidates.
Multifocal Lenses Multifocal lenses provide the benefits of simultaneous vision for presbyopes through extended depth of focus (EDOF). They can also be utilized for managing myopia progression. Multifocal contact lenses that have distance power in the center and near power in more peripheral portions of the lens have been shown to slow the progression of myopia.21 In a recent case series analysis with a distance-center EDOF multifocal contact lens, 91% of patients demonstrated a decreased annualized progression of 70% or greater compared to their progression rates prior to being fit with the lens.22
Although managing myopia is a multifactorial process with several variables, there are strategies that use contact lenses that can help practitioners to manage the rate of progression. Consider the above-mentioned contact lens options as a valuable part of a physician’s toolbox to manage these individuals.
CARE ABOUT PRESBYOPIA
Presbyopia is a condition that all practitioners manage on a daily basis. Not surprisingly, virtually 100% of presbyopic patients require refractive correction. You might expect that because so many require refractive correction that a larger percentage of presbyopes would wear contact lenses, yet only 7% of presbyopes over 50 years old currently wear them.23 From a clinical perspective, this is a large unmet need in eye care.
Part of the reason why this occurs may be that clinicians are not offering contact lenses as a viable option to presbyopes. And, if they are, they may not be explaining presbyopic contact lens options optimally. Practitioners need to be cautious about how they communicate with presbyopes about their options; most likely, a number of presbyopes would be interested in contact lens options if they were aware that they were candidates for them.
Remember to utilize all of the means at your disposal when treating presbyopes. Specialty lenses, including corneal GP and scleral lenses, provide a highly customized way to offer this correction. Hybrid multifocal lens options provide the advantage of GP optics with a soft skirt. Custom soft lenses in both hydrogel and silicone hydrogel materials provide multiple opportunities for even uncommon prescriptions. New multifocal astigmatic options available for immediate fittings provide a sharper visual experience for those who have low-to-moderate cylinder levels and who are either not currently corrected or have dropped out of multifocals in the past because of the uncorrected astigmatism. And, for those presbyopes who have spherical corrective needs, a plethora of daily disposable multifocal options currently exist. It is necessary to make presbyopes aware of these options and to customize their corrective needs.
CONCLUSION
Several advancements in recent years have given practitioners the opportunity to care for their patients in new ways with contact lenses. By embracing these options, practitioners are certain to take their contact lens practice to the next level. CLS
Editorial support for this article provided by Marc Deeley, OD, Medically Necessary Contact Lens Fellow, University of Illinois Eye and Ear Infirmary.
REFERENCES
- Brujic M. How important Is optical placement In multifocal lenses? Poster presented at the Global Specialty Lens Symposium, Las Vegas, Jan. 2015.
- Brujic M. Effects of line of sight on patients vision. Poster presented at the Global Specialty Lens Symposium, Las Vegas. Jan. 2016.
- Markoulli M, Kolanu S. Contact lens wear and dry eyes: challenges and solutions. Clin Optom (Auckl). 2017 Feb 15;9:41-48.
- Dumbleton K, Woods CA, Jones LW, Fonn D. The Impact of Contemporary Contact Lenses on Contact Lens Discontinuation. Eye Contact Lens. 2013 Jan;39:93-99.
- Pucker AD, Jones-Jordan LA, Marx S, et al; Contact Lens Assessment of Symptomatic Subjects (CLASS) Study Group. Clinical factors associated with contact lens dropout. Cont Lens Anterior Eye. 2019 Jun;42:318-324.
- Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017 Jul;15:575-628.
- Rynerson JM, Perry HD. DEBS – a unified theory for dry eye and blepharitis. Clin Ophthalmol. 2016 Dec 9:10:2455-2467.
- Karakurt Y, Zeytun E. Evaluation of the Efficacy of Tea Tree Oil on the Density of Demodex Mites (Acari: Demodicidae) and Ocular Symptoms In Patients With Demodectic Blepharitis. J Parasitol. 2018 Oct;104:473-478.
- Stroman DW, Mintun K, Epstein AB, et al. Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. Clin Opthalmol. 2017 Apr;11:707-714.
- Blackie CA, Coleman CA, Nichols KK, et al. A single vectored thermal pulsation treatment for meibomian gland dysfunction increases mean comfortable contact lens wearing time by approximately 4 hours per day. Clin Ophthalmol. 2018 Jan 17;12:169-183.
- Downie LE, Gad A, Wong CY, et al. Modulating contact lens discomfort with anti-inflammatory approaches: A randomized controlled trial. Invest Ophthalmol Vis Sci. 2018 Jul 2;59:3755-3766.
- Hom MM. Use of cyclosporine 0.05% ophthalmic emulsion for contact lens-intolerant patients. Eye Contact Lens. 2006 Mar;32:109-111.
- Gonzalez AL. Safety and efficacy of lifitegrast 5% ophthalmic solution in contact lens discomfort. Clin Ophthalmol. 2018;12:2079-2085.
- Giovagnoli D, Graham SJ. Inferior punctal occlusion with removable silicone punctal plugs in the treatment of dry-eye related contact lens discomfort. J Am Optom Assoc. 1992 Jul;63:481-485.
- Saw SM, Matsumura S, Hoang QV. Prevention and management of myopia and myopic pathology. Invest Ophthalmol Vis Sci. 2019 Feb 1;60:488-499.
- Prousali E, Haidich AB, Fontalis A, Ziakas N, Brazitkos P, Mataftsi A. Efficacy and safety of interventions to control myopia progression in children: an overview of systematic reviews and meta-analyses. BMC Ophthalmol. 2019 May 9;19:106.
- Weiss RS, Park S. Recent updates on myopia control: preventing progression 1 diopter at a time. Curr Opin Ophthalmol. 2019 Jul;30:215-219.
- Hiraoka T, Sekine Y, Okamoto F, Mihashi T, Oshila T. Safety and efficacy following 10-years of overnight orthokeratology for myopia control. Ophthalmic Physiol Opt. 2018 May;38:281-289.
- Na M, Yoo A. The effect of orthokeratology on axial length elongation in children with myopia: Contralateral comparison study. Jpn J Ophthalmol. 2018 May;62:327-334.
- Li X, Friedman IB, Medow NB, Zhang C. Update on Orthokeratology in Managing Progressive Myopia in Children: Efficacy, Mechanisms, and Concerns. J Pediatr Ophthalmol Strabismus. 2017 May 1;54:142-148.
- Zhu Q, Liu Y, Tighe S, et al. Retardation of myopia progression by multifocal soft contact lenses. Int J Med Sci. 2019 Jan 1;16:198-202.
- Cooper J, O’Connor B, Watanabe R, et al. Case Series Analysis of Myopic Progression Control With a Unique Extended Depth of Focus Multifocal Contact Lens. Eye Contact Lens. 2018 Sep;44:e16-e24.
- Caroll M, LaHiff J. Overcoming a Presbyopia Problem. Contact Lens Spectrum. 2009 Nov;24:33-35,54. Available at www.clspectrum.com/issues/2009/november-2009/overcoming-the-presbyopia-problem . Accessed Oct. 3, 2019.