



Radial keratotomy (RK) was the first popularized corneal refractive surgery for the correction of myopia. During the RK procedure, partial-thickness incisions are cut into the cornea in a radial pattern, which results in corneal flattening.
At its peak, approximately 250,000 RK procedures were performed annually in the United States (McDonald, 2011). Ten-year results from the Prospective Evaluation of Radial Keratotomy (PERK) study showed that of the 310 bilateral cases, 70% of patients reported not needing distance correction with glasses or contact lenses (Waring et al, 1994). However, many patients who have undergone RK become hyperopic; the PERK study stated that the refractive error of 43% of eyes changed in the hyperopic direction by 1.00D or more. Clinically, we know that some patients also have diurnal refractive fluctuations and corneal irregularity.
Contact Lens Challenges
Depending on the degree of flattening, post-RK corneas are significantly oblate. This can lead to failure when attempting to fit molded frequent-replacement soft contact lenses that are designed for prolate eyes. Corneal GP lenses are an option, but failure to precisely match to the surface profile will lead to failure.
Scleral lenses can provide a centered, stabilized fit by vaulting the oblate corneal surface. A reverse geometry design provides even corneal clearance. Paracentral areas of ectasia can increase the complexity of obtaining limbus-to-limbus vault.
Case in Point A 58-year-old patient who underwent eight-cut RK surgery in 1995 needed a scleral lens refit after recent cataract surgery for his right eye. A corneal elevation map of his right eye showed central flattening, with a paracentral inferior temporal area of ectasia (Figure 1a). Scleral topography measured significant asymmetry. A best-fit 16mm diagnostic scleral lens with a base curve of 45D used for over-refraction demonstrated bearing at the area of ectasia (Figure 1b).
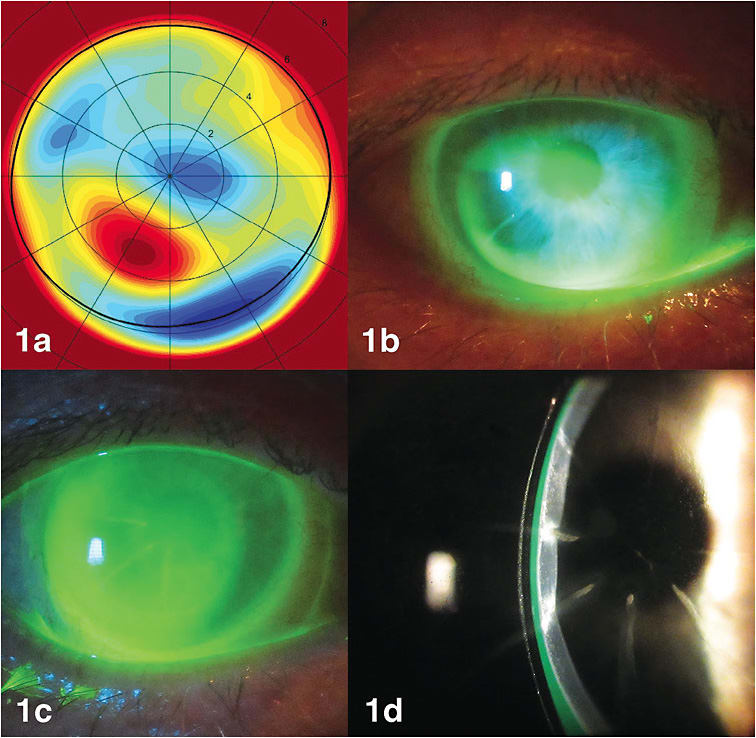
A free-form customized lens designed from corneo-scleral topography with a base curve of 34.25D evenly vaulted the flattened central cornea while clearing the area of ectasia (Figure 1c/1d). The patient achieved 20/30 vision with comfortable lens wear.
Monitoring
Frequent follow-up visits should be scheduled to monitor these patients for vascularization. Hypoxia-induced stress or mechanical trauma from a poorly fit scleral lens can result in the initiation of corneal blood vessels that can easily track along the corneal incisions, especially in ones that continue to the limbus. We used a GP material with a Dk of 200 for our patient to reduce the risk of vascular formation.
Conclusions
Scleral lenses can be an optimal lens choice for post-RK patients who require visual correction. They can provide a customized, stable fit that corrects the refractive error and can diminish diurnal refractive fluctuations during lens wear. CLS
For references, please visit www.clspectrum.com/references and click on document #288.