



Physiology is defined by Merriam-Webster’s medical dictionary as “a branch of biology that deals with the functions and activities of life or of living matter (as organs, tissues, or cells) and of the physical and chemical phenomena involved” and as “the organic processes and phenomena of an organism or any of its parts or of a particular bodily process.” Since the first scleral lenses appeared in the late 1800s, researchers have been interested in describing the effects of contact lenses on ocular physiology. In his inaugural dissertation on contact lenses, August Müller speculated that “a disturbance to the nourishment of corneal tissue” was responsible for visual haze and corneal cloudiness that developed after a short period of wear.1 Decades later, Miller and Carroll outlined a series of tests to detect corneal edema associated with scleral lens wear.2
Throughout the early to mid-20th century, symptoms of severe corneal edema were relatively easy to identify, and clinical signs of edema were observable even without the sophisticated imaging equipment available in modern ophthalmic practice. Perhaps because of the ease of observing corneal edema, many early papers that sought to describe the effects of contact lens wear on the structure and function of the anterior ocular surface focused primarily on the development of edema with contact lens wear.
A considerable body of literature continued to focus on corneal edema associated with contact lens wear even after corneal GP lenses and hydrogel lenses pushed scleral lenses out of mainstream practice. Lack of oxygen was identified as a major causative factor in corneal edema development, and critical oxygen levels necessary to avoid unacceptable levels of corneal swelling were proposed by Holden et al in 1984.3 Harvitt and Bonanno supplemented Holden’s work in 1999, publishing an update to Fatt’s mathematical model of oxygen tension distribution across the cornea and contact lens.4 In addition to corneal edema, hypoxia also was hypothesized to be an underlying cause of corneal structure and function changes, including limbal hyperemia,5 corneal vascularization,6 refractive changes,7 epithelial microcysts,8 endothelial changes,9 and bacterial binding to epithelial cells.10
Of particular concern was the finding that hypoxia could facilitate bacterial binding to corneal epithelial cells. During the 1980s and 1990s, reports of microbial keratitis associated with contact lens wear emerged.11,12 Perhaps the most influential microbial keratitis studies during this period were by Poggio13 and Schein14 in 1989. In these studies comparing extended wear to daily wear of contact lenses, the authors showed a five-fold increase in microbial keratitis incidence and a 3.90 to 4.21 relative risk of microbial keratitis.
The confluence of these two lines of research (effects of corneal hypoxia and contact lens-associated microbial keratitis) galvanized the ophthalmic community to find ways to increase oxygen supply to the cornea during contact lens wear. Based on research available in the late 1990s, the prevailing theory was that improving oxygen transmissibility (Dk/t: the lens oxygen permeability [Dk] divided by the lens thickness [t]) through a contact lens should reduce the microbial keratitis risk associated with contact lens wear. Silicone hydrogel contact lens materials were introduced with great fanfare in the late 1990s, and the ophthalmic community optimistically anticipated a significant reduction in contact lens-associated microbial keratitis and other hypoxia-related contact lens wear-related complications.
Results of post-marketing studies were disappointing. In 2005, Schein reported that microbial keratitis incidence in patients who wore silicone hydrogel lenses continuously for as many as 30 days was 18 per 10,000 patient years of wear.15 This was similar to the incidence that had been previously reported for extended-wear hydrogel lenses (20.9 per 10,000 patient years of wear13). Several years later, Radford reported that while silicone hydrogel contact lens wear eliminated hypoxia-related complications, it was associated with an increased risk of nonulcerative keratitis (referred to as “sterile” keratitis) and mechanically induced ocular surface disorders.16
As research into the effects of hypoxia on corneal integrity was developing, scleral lenses—which had never completely disappeared—were quietly making a comeback. The use of GP lens materials for fabricating scleral (or haptic) lenses provided an answer to the problem of corneal edema associated with polymethylmethacrylate (PMMA) scleral lenses. Throughout the 1990s, GP scleral lenses were developed and prescribed to treat severe corneal irregularity and ocular surface disease at tertiary care centers throughout the world. When scleral lenses were being prescribed primarily for patients who had severe eye disease, their benefits largely outweighed any potential risks. Scleral lenses allowed for re-epithelialization of persistent epithelial defects, protected the ocular surface in severe keratoconjunctivitis sicca, and allowed for the delay or even avoidance of aggressive surgical intervention in patients who had primary or secondary corneal ectasia.
As scleral lenses have become commercially available, indications for their use are expanding to include less severe ocular pathology. Scleral lenses are now prescribed for mild-to-moderate corneal irregularity, ocular surface disease, and even for uncomplicated refractive error. Assessing the risks and benefits of scleral lens wear in patients who do not have severe ocular pathology requires a more thorough understanding of how scleral lenses can affect anterior ocular physiology. Given the emphasis on corneal hypoxia in contact lens research, it is not surprising that oxygen transmissibility through both a scleral lens and the post-lens fluid reservoir is currently a focus of investigation.
THEORETICAL MODELS FOR PREDICTING CORNEAL SWELLING DURING SCLERAL LENS WEAR
There are a few theoretical models in the literature for predicting corneal hypoxia associated with scleral lens wear, and clinical recommendations have been made accordingly. For example, Michaud et al18 suggested prescribing lenses with a Dk of more than 150 barrers, central lens thickness of less than 250μm, and a central post-lens tear thickness (PoLTT) below 200μm to avoid hypoxia-induced swelling, based on Fatt’s method of combining oxygen transmissibilities (Dk/t).17 Compañ et al19 suggested using scleral lenses with Dk greater than 125 barrers, central lens thickness of less than 200μm, and a PoLTT below 150μm to avoid corneal swelling by predicting the oxygen tension profile due to oxygen consumption and diffusion.20 Using a different theoretical model, Jaynes et al drew similar conclusions and stated that only scleral lenses made from the highest-Dk material and fitted without an excessive tear reservoir depth might avoid corneal swelling.21 These theoretical models recommend that clinicians design scleral lenses with the highest-Dk materials and the thinnest post-lens tear reservoirs, despite several clinical studies22,23 reporting only 0.68% to 1.8% corneal edema for healthy subjects during scleral lens wear. This is less than the 2% to 4% normal physiological swelling that results from the hypoxia induced by overnight eye closure without contact lenses.24,25
The direct relationship between hypoxia and corneal swelling cannot be accurately predicted with these theoretical models without including aerobic and anaerobic glucose-consumption reactions. A recent theoretical model by Kim et al considered the effects of corneal metabolites, membrane metabolic transport resistance, and corneal stromal thickness-hydration relations26 to predict edema induced by hypoxia. These authors suggested that within practical ranges of lens oxygen transmissibility (e.g., Dk/t of 20 to 40 hectobarrers/cm) and post-lens tear reservoir thickness (e.g., 50µm to 400μm), the influences of both lens material Dk and tear reservoir depth were minimal (i.e., no more than 2% corneal swelling). Specifically, the authors found that a scleral lens with a Dk/t of less than 10 hectobarrers/cm induced more than the physiologically normal overnight no-lens-wear swelling, regardless of the post-lens tear reservoir thickness. Fortunately, with modern scleral lens fitting, we do not need to worry about using low-Dk lens materials, as GP lens materials are readily available.
Of interest, in an open-eye lens wear condition, for a scleral lens with a typical settled PoLTT ranging from 50µm to 400µm and lens Dk/t within the range of 20 to 40 hectobarrers/cm, corneal swelling was predicted to be less than 2%.26 Additionally, there is minimal to no additional benefit in further reducing corneal swelling once the lens material reaches a Dk/t level greater than 45 hectobarrers/cm, according to Kim et al’s predictions.26
In the closed-eye condition, however, a significant amount of corneal swelling (i.e., well above 4%) was predicted, even with lens materials that offer a Dk/t greater than 45 hectobarrers/cm.26 These predictions suggest that when the cornea is hypoxic (i.e., during eye closure), both lens material properties, such as Dk, and post-lens tear reservoir thickness contribute more to corneal edema compared to when the cornea is not deprived of oxygen (i.e., during open-eye lens wear). It is important to note that even if the highest-Dk lens material is used and the scleral lens fit creates the thinnest possible tear reservoir, it will not prevent a young lens wearer who has healthy corneas from having a significant amount of corneal swelling under closed-eye conditions. Thus, scleral lens wear during sleep is not recommended.
IN VIVO EFFECTS OF SCLERAL LENS DK/T AND POST-LENS TEAR CLEARANCE ON CORNEAL EDEMA
The predictions and recommendations made by Kim et al’s model26 are supported by recent clinical studies that examined the effects of lens Dk/t and the depth of the post-lens tear reservoir on corneal edema during scleral lens wear for young wearers who have healthy corneas.27,28,29 These studies showed that corneal swelling increased during the first one-and-a-half to two hours, reaching a plateau thereafter. At the end of five hours of lens wear, the mean corneal swelling was no more than 1.5%. The time course of corneal edema induced by scleral lens wear in this study was similar to those reported by Vincent et al, who further showed that it would take up to three hours after lens removal for the corneal thickness to restore to its baseline.22,30 Because it takes several hours for the cornea to recover from the physiological swelling during sleep, it may be prudent to recommend scleral lens application at least two hours after awakening and lens removal several hours before sleep. It is important to note that to date, there is no prospective study that offers additional insight about the clinical impact of “less than 2% corneal swelling” on the ocular surface health for patients who have healthy or diseased corneas.
Tan et al showed that there was no relationship between corneal swelling and lens Dk/t values ranging from 21 to 47 hectobarrers/cm.27 Additionally, the same authors showed no statistically significant correlation between corneal swelling and settled post-lens tear reservoir depth over a range of 65µm to 400µm, suggesting that achieving a scleral lens fit with a low clearance (e.g., ~200µm) may not necessarily provide an additional reduction in corneal swelling during lens wear. This finding initially was somewhat surprising, considering that oxygen availability at the corneal surface is related to the oxygen transmissibility of the combined system of a scleral lens and its post-lens tear film. It is important to note, however, that oxygen tension at the corneal surface is not directly related to corneal metabolism. As oxygen consumption rate is not linearly correlated with oxygen availability,26 it is not surprising that a linear change in tear clearance thickness does not result in a linear increase in corneal edema. Recent studies also reported conflicting findings with respect to the influence of the post-lens tear reservoir depth or tear clearance on corneal swelling. For example, Tan et al28 found no significant association between corneal edema and tear clearance, while Compañ et al20 reported a significant relationship. The discrepancy may be due in part to the latter study not accounting for lens Dk/t and not directly measuring the settled post-lens tear thickness.
IN VIVO POST-LENS TEAR DYNAMICS UNDER SCLERAL LENSES
Tear dynamics under a contact lens include tear exchange between the pre- and post-lens tears that occurs primarily at the lens periphery, tear mixing under the contact lens, and changes in post-lens tear thickness due to lens settling. Previous studies provided indirect evidence that efficient tear exchange with both soft and GP lenses can help preserve ocular surface integrity during sleep, making for safer overnight lens wear with these conventional lens types.31,32 With soft and GP lenses, it is hypothesized that fresh tears can resupply the anterior ocular surface with oxygen and other metabolites as well as components of immune defense, while at the same time remove cellular debris and dilute inflammatory mediators. In other words, sufficient tear exchange potentially can reduce biochemical and biophysical alterations due to tear stagnation during lens wear. Knowledge of the post-lens tear dynamics for soft or GP lenses may not be applicable to scleral lenses, as the on-eye lens fits vary among the different lens types. Specifically, scleral lenses have much more limited tear exchange, as well as a much longer settling time, compared to both soft and GP lenses.33,34 Recent studies show that scleral lens settling could continue throughout an entire five hours of lens wear, although the process appears to slow after four hours.22,29 It has been suggested that if a clinician’s goal is to maintain a minimum of 100µm of central tear clearance after five hours of lens settling, he or she would need a > 30% buffer at lens application by having the initial central tear clearance be no less than 145µm.28
With recent and emerging research technologies, clinicians can investigate post-lens tear dynamics during scleral lens wear. Tse et al reported that roughly 30% of small-diameter scleral lens wearers have no observable tear exchange, while the remaining 70% exhibit both tear exchange and mixing.35 Post-lens tear mixing during scleral lens wear, which may be induced by natural convection in the post-lens tear compartment, has not been investigated quantitatively to date. It has been hypothesized that the less-than-expected corneal swelling reported in the studies discussed in this article may be partly the result of greater tear mixing due to convection in a relatively thicker tear reservoir, providing additional oxygen to the central cornea.35 Additional research is warranted to further our understanding of the roles of post-lens tear exchange and tear mixing in scleral lens wear safety.
CLINICAL CASES
Despite predictions that corneal hypoxia will occur with scleral lenses that are fit with more-than-minimal corneal clearance, many cases of long-term scleral lens wear challenge this notion. In most studies, the edema reported, even with higher clearances, is below even the physiologically normal edema that results from eye closure and sleep-related hypoxia. In addition to tear clearance, other factors that are likely to play a role in physiological function during scleral lens wear include lens diameter, oxygen transmissibility, amount of tear exchange or mixing, lens suction, and any effects of improper fit on the ocular surface. Generalizing one lens attribute as the main source of complications may result in overlooking the actual causes and thus may hinder proper troubleshooting.
The purpose of these clinical cases from long-term scleral lens wearers is to demonstrate that there are perhaps other factors and parameters that are important to consider when aiming to achieve adequate physiological endpoints in a scleral lens fit. More studies are needed to look further into the effects of lens diameter, tear-exchange, and lens suction.
Sjögren’s Syndrome Patient A 69-year-old female was referred for scleral lens fitting in February 2008. She was diagnosed with Sjögren’s syndrome approximately six years earlier and was experiencing considerable ocular discomfort despite punctal occlusion, use of moisture chamber glasses, and use of nonpreserved artificial tears up to 10 times daily. Her entering visual acuity was 20/25 OD, 20/20 OS.
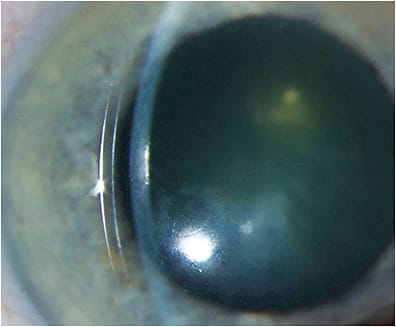
She was fitted with 17.5mm scleral lenses in both eyes (Boston XO2 [Bausch + Lomb], Dk ~140). She reported an immediate improvement in comfort and achieved 20/20 acuity in each eye with the lenses. The right lens had 470 microns of central clearance, and the left lens showed 450 microns of central clearance (Figure 1). Corneal thickness at baseline was 546 microns OD and 556 microns OS.
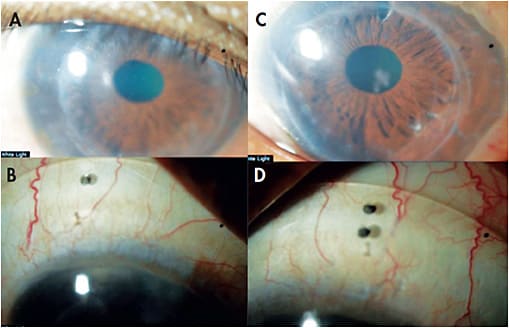
At her most recent visit (November 2018), central corneal thickness was 545 microns OD and 554 microns OS. The corneas remain clear, with no signs of edema, endothelial cell dysfunction, or vascularization (Figure 2).

Longstanding Grafted Patient A 61-year-old female who had a history of keratoconus had undergone penetrating keratoplasty in both eyes approximately 40 years prior. She was fitted 11 years ago with scleral lenses (19.5mm OD and 20mm OS, Boston XO2) secondary to corneal GP lens intolerance (Figure 3). Entering best-corrected visual acuity with corneal GPs was in the 20/40 range OD/OS, improving to 20/20 OD/OS with the scleral lenses.
Both grafts appeared clear and compact at baseline, with an average thickness of 549µm OD and 687µm OS (ultrasound pachymeter). Endothelial cell count was 1,167 cells/mm2 OD and 840 cells/mm2 OS (confocal microscope). In accordance with our fitting philosophy in 2008, the lenses were fit to distribute the weight over a large surface area, to ensure complete clearance over the entire cornea and limbus, to rule out any signs of conjunctival impingement or compression beneath the haptic zone, to ensure that there was no edge imprint or staining on the conjunctiva after lens removal, and to allow for tear exchange to promote fluid ventilation.
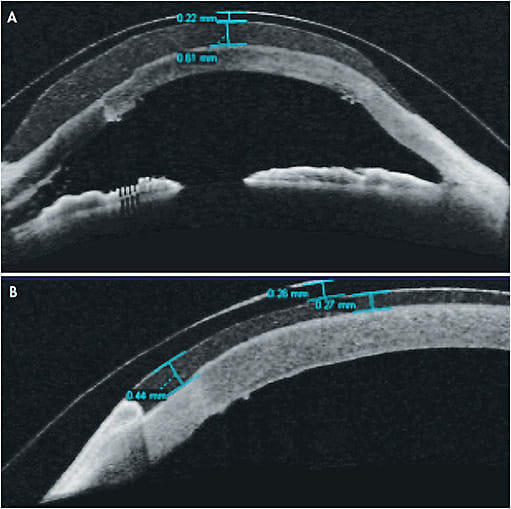
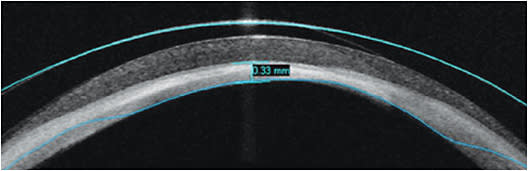
After 11 years of scleral lens wear, best-corrected visual acuity continued to be 20/20 for each eye, and average pachymetry was at 554µm OD and 681µm OS (Pentacam, Oculus), with no objective or subjective clinical signs of microcystic epithelial edema, Sattler’s veil, or vascularization. Optical coherence tomography (OCT) images revealed a central tear clearance of ~600µm OD and ~250µm OS. The central lens thickness was ~220µm OD and ~226µm OS (Figure 4).
Longstanding Stevens-Johnson Syndrome (SJS) Patient A 44-year-old female who had a history of SJS has been a monocular patient, with only light perception in the right eye, for more than 20 years. She was fitted with scleral lenses in 2006. Despite severe disease progression over the years, best-corrected vision in her left eye remained between 20/30 and 20/40 (fluctuation due to post-lens fluid reservoir debris) for 12 years, until late 2018. The patient needed to remove and re-apply the lens one-to-two times per day to manage the debris. She was wearing a 19.5mm, eight-meridian custom scleral lens in Boston XO2 material (Figure 5), and our fitting goals were to maintain complete clearance over the cornea and limbal area 360º degrees around, to avoid limbal compression, and to allow generous and homogenous lens weight distribution over the conjunctival tissue overlying the sclera. We ruled out signs of impingement or compression by confirming no lens or edge imprint or conjunctival staining after lens removal. We also monitored and ruled out subjective or objective signs of edema.

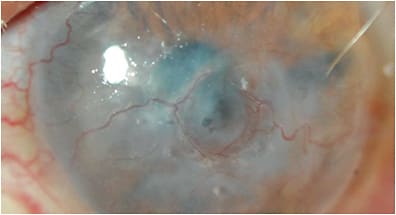
In an attempt to eliminate post-lens tear reservoir debris, the patient was refit elsewhere into a 16mm lens. This lens settled during wear, causing corneal touch and mechanical rubbing, which resulted in a persistent epithelial defect. Given her cornea’s fragile state and limbal stem cell deficiency secondary to SJS, the epithelial defect progressed to a full corneal melt, which required glue to stabilize the cornea. After the surface was stabilized, she returned to our clinic to re-attempt a larger scleral lens, with the goal to protect the ocular surface. Given the delicate state of the corneal epithelium, evaluation at her new baseline showed microcystic epithelial edema and bullae with scleral lens wear. There also was a circumferential ring of vascularization (feeder vessels) around the area where the melt had occurred and increased haze (Figure 6). Best-corrected vision entering with a scleral lens at that time was 20/80.
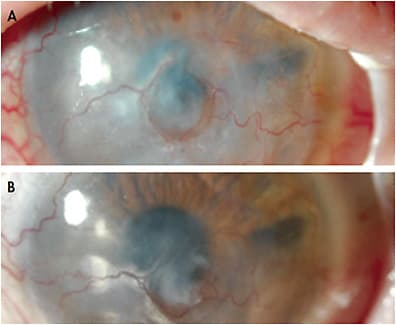
The patient was refitted to address adequate physiological function and to avoid bullae and edema. The lens diameter was kept at 19.5mm, with Boston XO2 material and center thickness of ~250µm; two ventilating channels were added at 3 o’clock and 9 o’clock on the lens as well as a haptic fenestration at the 12 o’clock location. The ventilating channels were incorporated to promote tear exchange and to reduce lens suction. The central tear clearance as estimated by OCT remained at ~600µm (Figure 7). After making these lens fit changes, there were no more signs or symptoms of microcystic corneal edema or bullae, and vision improved to 20/50 (Figure 8A). After only four months of wear, follow-up evaluation showed continuous ocular surface improvement, with no onset of microcystic edema or bullae and improvement in vision to ~20/30 (back to the baseline prior to the corneal melt), with some mild evidence of haze clearing and vascularization reduction (Figure 8B). In this case of complex ocular surface disease, a smaller-diameter scleral lens with minimal clearance actually caused a complication that was remedied by a large-diameter scleral lens that emphasized planned fluid ventilation to maximize oxygen availability to the cornea, avoid a tight lens fit, and eliminate suction as well as providing even lens distribution over a large surface area despite having ample tear clearance. These sets of variables, as shown in Figure 8B, have provided optimal physiological and visual outcomes for this patient.
CONCLUSION
The disparity between predicted and reported hypoxia complications of scleral lens wear may suggest that decreased oxygen transmission through the lens/reservoir complex is not the only factor that we must consider when evaluating the effects of scleral lens wear on anterior ocular physiology. The role of suction, tear exchange, and limbal clearance in scleral lens wear should be considered and further investigated. To properly discern the causes of observed complications, more controlled experiments and clinical studies are required. Variables such as lens diameter, haptic “weight” or pressure distribution, corneal clearance, and tear exchange must be considered as our study of the physiologic effects of scleral lenses on ocular surface tissue continues. CLS
REFERENCES
- Pearson RM, Efron N. Hundredth anniversary of August Müller’s inaugural dissertation on contact lenses. Surv Ophthalmol. 1989 Sep-Oct;34:133-141.
- Miller D, Carroll JM. Corneal edema and scleral lenses. Int Ophthalmol Clin. 1968 Fall;8:623-635.
- Holden BA, Mertz GW. Critical oxygen levels to avoid corneal edema for daily and extended wear contact lenses. Invest Ophthalmol Vis Sci. 1984 Oct;25:1161-1167.
- Harvitt DM, Bonanno JA. Re-evaluation of the oxygen diffusion model for predicting minimum contact lens Dk/t values needed to avoid corneal anoxia. Optom Vis Sci. 1999 Oct;76:712-719.
- Papas E. On the relationship between soft contact lens oxygen transmissibility and induced limbal hyperaemia. Exp Eye Res. 1998 Aug;67:125-131.
- Dumbleton KA, Chalmers RL, Richter DB, Fonn D. Vascular response to extended wear of hydrogel lenses with high and low oxygen permeability. Optom Vis Sci. 2001 Mar;78:147-151.
- Binder PS. Myopic extended wear with the Hydrocurve II soft contact lens. Ophthalmology. 1983 Jun;90:623-626.
- Holden BA, LaHood D, Sweeney DF. Prediction of extended wear microcyst response on the basis of mean overnight corneal response in an unrelated sample of non-wearers. Am J Optom Physiol Opt. 1987;64[Suppl]:83.
- Holden BA, Williams L, Sweeney DF, Swarbrick HA. The endothelial response to contact lens wear. CLAO J. 1986 Jul-Sep;12:150-152.
- Cavanagh HD, Ladage P, Yamamoto K, Li SL, Petroll WM, Jester JV. Effects of daily and overnight wear of hyper-oxygen transmissible rigid and silicone hydrogel lenses on bacterial binding to the corneal epithelium: 13-month clinical trials. Eye Contact Lens. 2003 Jan;29(1 Suppl):S14-16; discussion S26-29, S192-194.
- Galentine PG, Cohen EJ, Laibson PR, Adams CP, Michaud R, Arentsen JJ. Corneal ulcers associated with contact lens wear. Arch Ophthalmol. 1984 Jun;102:891-894.
- Dart JK. Predisposing factors in microbial keratitis: the significance of contact lens wear. Br J Ophthalmol. 1988 Dec;72:926-930.
- Poggio EC, Glynn RJ, Schein OD, et al. The incidence of ulcerative keratitis among users of daily-wear and extended-wear soft contact lenses. N Engl J Med. 1989 Sep 21;321:779-783.
- Schein OD, Glynn RJ, Poggio EC, Seddon JM, Kenyon KR. The relative risk of ulcerative keratitis among users of daily-wear and extended-wear soft contact lenses. A case-control study. Microbial Keratitis Study Group. N Engl J Med. 1989 Sep 21;321:773-778.
- Schein OD, McNally JJ, Katz J, et al. The incidence of microbial keratitis among wearers of a 30-day silicone hydrogel extended-wear contact lens. Ophthalmology. 2005 Dec;112:2172-2179.
- Radford CF, Minassian D, Dart JK, Stapleton F, Verma S. Risk factors for nonulcerative contact lens complications in an ophthalmic accident and emergency department: a case-control study. Ophthalmology. 2009 Mar;116:385-392.
- Michaud L, van der Worp E, Brazeau D, Warde R, Giasson CJ. Predicting estimates of oxygen transmissibility for scleral lenses. Cont Lens Anterior Eye. 2012 Dec;35:266-271.
- Fatt, I. Oxygen-transmissibility considerations for a hard-soft contact lens combination. Am J Optom Physiol Opt. 1977 Oct;54:666-672.
- Compañ V, Oliveira C, Aguilella-Arzo M, Mollá S, Peixoto-de-Matos SC, González-Méijome JM. Oxygen diffusion and edema with modern scleral rigid gas permeable contact lenses. Invest Ophthalmol Vis Sci. 2014 Sep 4;55:6421-6429.
- Chhabra M, Prausnitz JM, Radke CJ. Modeling corneal metabolism and oxygen transport during contact lens wear. Optom Vis Sci. 2009 May;86:454-466.
- Jaynes JM, Edrington TB, Weissman BA. Predicting scleral GP lens entrapped tear layer oxygen tensions. Cont Lens Anterior Eye. 2015 Feb;38:44-47.
- Vincent SJ, Alonso-Caneiro D, Collins MJ. Corneal changes following short-term miniscleral contact lens wear. Cont Lens Anterior Eye. 2014 Dec;37:461-468.
- Vincent SJ, Alonso-Caneiro D, Collins MJ, et al. Hypoxic corneal changes following eight hours of scleral contact lens wear. Optom Vis Sci. 2016 Mar;93:293-299.
- Mertz GW. Overnight swelling of the living human cornea. J Am Optom Assoc. 1980 Mar;51:211-214.
- Graham AD, Fusaro RE, Polse KA, Lin MC, Giasson CJ. Predicting extended wear complications from overnight corneal swelling. Invest Ophthalmol Vis Sci. 2001 Dec;42:3150-3157.
- Kim YH, Tan B, Lin MC, Radke CJ. Central corneal edema with scleral-lens wear. Curr Eye Res. 2018 Nov;43:1305-1315.
- Tan B, Tse V, Kim YH, Lin K, Zhou Y, Lin MC. Effects of scleral-lens oxygen transmissibility on corneal thickness: A pilot study. Cont Lens Anterior Eye. 2019 Apr 15. [Epub ahead of print]
- Tan B, Zhou Y, Yuen TL, Michaud L, Lin K, Lin MC. Effects of scleral-lens tear clearance on corneal edema and post-lens tear dynamics: A pilot study. Optom Vis Sci. 2018 Jun;95:481-490.
- Vincent, SJ, Alonso-Caneiro, D, Collins, MJ. The temporal dynamics of miniscleral contact lenses: central corneal clearance and centration. Cont Lens Anterior Eye. 2018 Apr;41:162-168.
- Vincent SJ, Alonso-Caneiro D, Collins MJ. The time course and nature of corneal oedema during sealed miniscleral contact lens wear. Cont Lens Anterior Eye. 2019 Feb;42:49-54.
- Lin MC, Yeh TN, Graham AD, et al. Ocular surface health during 30-day continuous wear: rigid gas-permeable versus silicone hydrogel hyper-o2 transmitted contact lenses. Invest Ophthalmol Vis Sci. 2011 Jun 1;52:3530-3538.
- Lin MC, French HM, Graham AD, Sanders TL. Effects of daily irrigation on corneal epithelial permeability and adverse events with silicone hydrogel contact lens continuous wear. Invest Ophthalmol Vis Sci. 2014 Feb 10;55:776-783.
- Paugh JR, Chen E, Heinrich C, et al. Silicone hydrogel and rigid gas-permeable scleral lens tear exchange. Eye Contact Lens. 2018 Mar;44:97-101.
- Tan B, Yuen TL, Moy A, et al. Pilot study of post-lens fluorogram with scleral lenses of various clearances. Presented at American Academy of Optometry 2015, New Orleans.
- Tse V, Tan B, Kim YH, Zhou Y, Lin MC. Tear dynamics under scleral lenses. Cont Lens Anterior Eye. 2019 Feb;42:43-48.