



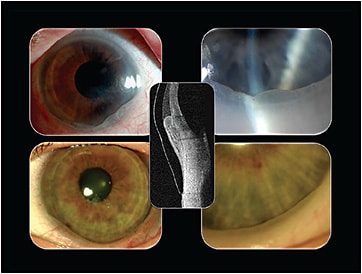
In certain scleral lens wearers, the conjunctiva can become prolapsed under the lens (Figure 1). In this situation, the atmospheric pressure outside of the scleral lens is greater compared to the pressure beneath the lens, resulting in a closed negative pressure system (suction force). This raises concerns about the potential for an increase in intraocular pressure (IOP) in some scleral wearers. We studied this using a tonometer that measures IOP transpalpebrally, through the upper eyelid, while scleral lenses are worn (Figure 2).

Methods
This study was approved by the Pacific University human research ethics committee and adhered to the tenets of the Declaration of Helsinki. Fourteen normal-eye subjects were fitted with two different commercially available scleral lens designs, ranging in diameter from 14.6mm to 15.2mm. Subjects’ baseline IOP was measured with the Diaton Tonometer (BiCom, Inc.) at both 8:00 am and 4:00 pm.
The following day, the first pair of scleral lenses was applied at 8:00 am. IOP was measured with the Diaton immediately after lens application and then again after eight hours of wear. The lenses were then removed and the IOP immediately measured. This procedure was then repeated the following week with the second pair of scleral lenses.
Results
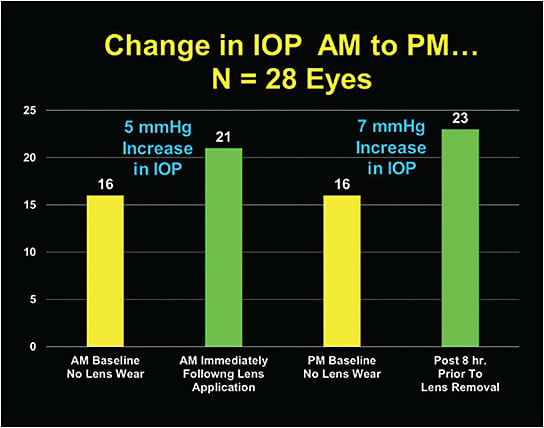
Figure 3 shows that immediately following lens application, IOP increased (above baseline) an average of 5.0 mmHg. All subjects showed an increase in IOP, and the increase was not significantly different between the two study lens designs. The difference between the baseline 4:00 pm IOP and the IOP after eight hours of scleral lens wear was 7.0 mmHg for both designs. Additionally, 11 of the 28 eyes had increases in IOP of 10 mmHg or greater following eight hours of lens wear.
Discussion
Upon scleral application, IOP increased in all subjects and appeared to remain elevated throughout the wearing period. The IOP immediately returned to baseline following lens removal. This suggests that the suction force beneath the lens may be the primary contributor to the IOP changes. However, we cannot rule out other anatomical factors.
Conclusion
These data raise important clinical questions: 1) What are the long-term consequences of increased IOP with scleral wear? 2) How much IOP increase, if any, is acceptable? 3) Are the suction forces similar among various diameters/designs? 4) Should we market sclerals for patients who would succeed in other lens types? 5) Can any design modifications decrease the suction forces? CLS
The authors thank Steve Turpin, OD, and Kennedy Antoniuk, OD, for their assistance with this study.