


This course is COPE approved for 2 hours of CE credit and NCLE General Knowledge approved for 1 hour of CE credit.
COPE Course ID: 66350-CL NCLE Course ID: CWCLS002
Release Date: April 1, 2020 Expiration Date: January 17, 2023

LEARNING METHOD AND MEDIUM
This educational activity consists of a written article and 20 study questions. The participant should, in order, read the Activity Description listed at the beginning of this activity, read the material, answer all questions in the post test, and then complete the Activity Evaluation/Credit Request form.
To receive credit for this activity, please follow the instructions provided below in the section titled To Obtain CE Credit. This educational activity should take a maximum of 2 hours to complete.
CONTENT SOURCE
This continuing education (CE) activity captures key statistics and insights from contributing faculty.
ACTIVITY DESCRIPTION
The goal of this article is to better eyecare professionals’ understanding of scleral lenses, techniques and technologies for fitting, lens design, approaches to irregularities and obstacles, and a discussion surrounding guides and lens modification.
A review of the literature will provide the reader with a better understanding of various instrumentation, scleral lens prescriptions, and fitting techniques.
TARGET AUDIENCE
This educational activity is intended for optometrists, contact lens specialists, and other eyecare professionals.
ACCREDITATION DESIGNATION STATEMENT
This course is COPE approved for 2 hours of CE credit and NCLE General Knowledge approved for 1 hour of CE credit.
COPE Course ID: 66350-CL
NCLE Course ID: CWCLS002
DISCLOSURES
Jennifer Swingle Fogt, OD, MS, has received research funding and honorarium from Alcon and Contomac, research funding from Nevakar, Ocugen, and Shire, honorarium from NovaSight, and consulting fees from EyeLab.
Chad Rosen, OD, MBA, editor of the continuing education series, has nothing to disclose.
DISCLOSURE ATTESTATION
The contributing faculty member has attested to the following:
- That the relationships/affiliations noted will not bias or otherwise influence her involvement in this activity;
- That practice recommendations given relevant to the companies with whom she has relationships/affiliations will be supported by the best available evidence or, absent evidence, will be consistent with generally accepted medical practice;
- That all reasonable clinical alternatives will be discussed when making recommendations.
TO OBTAIN CE CREDIT
To obtain COPE CE credit for this activity, read the material in its entirety and consult referenced sources as necessary. We offer instant certificate processing for COPE credit. Please take the post test and evaluation online by using your OE tracker number and logging in to clspectrumce.com .
Upon passing the test, you will immediately receive a printable PDF version of your course certificate for COPE credit. On the last day of the month, all course results will be forwarded to ARBO with your OE tracker number and your records will be updated. You must score 70% or higher to receive credit for this activity. Please make sure you take the online post test and evaluation on a device that has printing capabilities.
To obtain NCLE credit, a score of 80% or higher is required. Passing scores will be forwarded to ABO-NCLE at the end of each month.
NO-FEE CONTINUING EDUCATION
There are no fees for participating in and receiving credit for this activity.
DISCLAIMER
The views and opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of NOVA Southeastern University College of Optometry or Contact Lens Spectrum. This CE activity is copyrighted to PentaVision LLC ©2020. All rights reserved.
This continuing education activity is supported by unrestricted grants from ABB Optical Group, Blanchard Contact Lenses, BostonSight, Menicon, and X-Cel Specialty Contacts.
RELEASE DATE: APRIL 1, 2020
EXPIRATION DATE: JANUARY 17, 2023
To view this CE activity in its entirety and proceed to the test, visit clspectrumce.com
Scleral contact lenses have been growing in popularity among practitioners and patients for their ability to provide stable vision and comfort. They are particularly useful for patients who have irregular corneas, but their use is also increasing in patients who have ocular surface disorders and refractive error.1 Scleral lens fitting can be approached in a number of ways, including using fitting sets or different instruments to help select an initial lens. The need to vault the entire cornea such that the lens rests on the scleral surface introduces multiple variables to consider when refining a lens fit. As with all contact lens fits, the initial lens chosen for a patient is not always the final one selected. While there is variation in the parameters that successful practitioners use to fit scleral lenses,1 there are overall guidelines that apply to fitting all lenses.
REVIEW OF BASIC COMPONENTS
Before discussing how to fine-tune a scleral lens fit, a review of the basic components of a fitting is needed. Initially, lenses are selected to ensure that they adequately vault over both the cornea and the limbus. Each lens fitting guide has specific instructions on how to select the first lens to try, with some sets defining lenses by their sagittal depth, base curve, or other characteristics. Key elements, such as an assessment of both central and limbal clearance as well as an examination of the edge fit in relation to the scleral surface, are critical to examining a scleral lens fit on the eye.
When using a diagnostic fitting set, it is important to first find a lens that vaults over the cornea and limbus adequately, then proceed to assessing the midperiphery and the edge of the lens fit, looking for obstacles or areas that prevent successful landing on the sclera. In general, finding a lens with enough depth to vault the cornea and limbus is the easiest part of the fitting, and central vaulting can be controlled by changing the base curve or peripheral curves that extend concentrically around the lens. However, difficulties can arise when a lens does not rest gently upon the sclera. Basic changes, such as flattening or steeping the outermost zone of the lens, can sometimes improve the fit, but the changes needed to fit this landing zone are more complicated than a singular change in curvature. Fortunately, many scleral lens designs now offer greater ability to refine lens edges and curves at multiple positions, allowing practitioners to fit many difficult eyes.
In this course, aspects of scleral lens fitting—including when to use special scleral lens design options, what technology is available to help determine which options to use, and how to use these designs to best care for your scleral lens patients—will be covered.
AVOIDING OBSTACLES
One of the great benefits of fitting a scleral lens is the ability to artfully “dodge” the irregularity of the cornea. For example, a large decentered cone of a keratoconic eye can interact with a corneal contact lens, causing the lens to rock and move excessively. When using a large scleral lens, these corneal obstacles can essentially be bypassed, assuming the fit creates enough clearance to vault over the challenging areas. This is a great help when dealing with corneal irregularities, and as a result, many practitioners are embracing this positive quality of scleral lenses.
Central scleral lens fit refinement requires practitioners to balance maintaining adequate clearance over the entire cornea without creating excessive vault. Excessive vault has been hypothesized to contribute to decreased oxygen transmissibility, also known as hypoxia. Oxygen must pass through both the thickness of the lens material and the entire tear lens created by the tears between the lens and the ocular surface.2 According to mathematical calculations, using materials with high oxygen permeability (Dk > 150), limiting lens thickness to 250µm, and limiting central lens clearance to less than 200µm will minimize hypoxia-related corneal swelling.2
Likewise, vaulting over the limbus is crucial, as this area is home to corneal stem cells. Studies have shown that it is important to maintain clearance in this area not only because of concerns about hypoxia, but also because mechanical interaction between a scleral contact lens and the limbus can cause corneal changes, such as corneal bullae, even in a short period of time.3 On the other hand, excessive clearance in this area can also be associated with conjunctival billowing or chalasis. So adequate, but not excessive, clearance at the limbus is required.
Optimizing scleral lens fit is generally handled by using a diagnostic fitting set and refining different curvatures of the lenses to raise or lower the sagittal height where needed. In general, diagnostic lens sets include guides that explain the changes required to achieve the desired clearances and edge qualities. Consultants are available to help with changes based on examiner observations, and the best lens designs are those in which a practitioner knows and can manage all lens parameters with or without assistance. Although I sometimes tell patients that scleral lenses are similar to “putting a bucket over the cornea” to make a new front surface, I explain that it is necessary to fit these lenses precisely to minimize short- and long-term complications and to maximize comfort.
Although critical to good vision and ocular health, achieving clearance over the cornea and the limbus is not the only factor important in a successful scleral lens fit. Fitting a lens that rests on the sclera but does not fit too tightly, nor impinge upon the underlying blood vessels, is important both for ocular health and for ease of lens removal by the patient. A lens that fits loosely, for example, could create discomfort and even inflammation due to excessive movement. Fitting the sclera is achieved by adjusting the haptic portion, or landing zone, of the lens in such a way that the entire zone rests evenly, distributing the weight of the lens without excessive impingement or edge lift.4 Utilizing a diagnostic lens set is a common method for assessing both clearance and lens edge, and these sets generally include lenses of varying sagittal height and edge lift. However, difficulties can arise when the sclera is not spherical or when obstacles are present where the lens is designed to rest. Knowing how to troubleshoot these problems can make scleral lens fitting a better experience for both practitioners and patients.
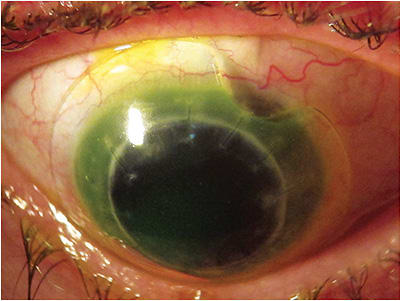
One common complication in fitting a scleral contact lens is literally a scleral obstacle. If a scleral lens is fit on an eye with a large pinguecula that sits just under the edge of the lens, the result may be impingement on the pinguecula, which in turn can cause irritation and discomfort (Figure 1).

When a lens fits well everywhere except for over the impediment, utilizing edge notching can be an option for solving this problem.
Laboratories may have variations on how this is best accomplished. Most, but not all, laboratories require a lens to be rotationally stable before a notch is added to the edge. While some designs utilize prism ballasting to stabilize a lens, the majority of lenses prevent rotation by adding toricity to the landing zone or haptic portion of the scleral lens. Preventing rotation of a lens that has a notch is important and is particularly critical if compression of a filtering bleb is to be avoided. A discussion of methods to determine how to best add toricity will occur later in this article.
In general, notching involves allowing the scleral lens to settle on the eye and then marking it for modification. Marks are placed on the edge of the lens on each side of the impediment, and then a third mark is placed (the dots should form a triangle) on the lens surface where the inward notch (toward the pupil) should end. Sending this lens back to the lab for creation of the notch should result in a custom lens that sits nicely on the sclera without discomfort. Some practitioners may be experienced enough to modify this notch themselves, but only if they have the proper equipment and routinely modify GP lenses. Once the custom lens is ready, patients should be instructed on how to apply the lens so that the notch is oriented in the correct position (Figure 2).
When an obstacle on the ocular surface is not at the edge of the lens but is interfering with the landing zone or peripheral portions of the lens, several options are possible for modifying it to vault the area. Each laboratory has a different strategy for handling these types of impediments, and one example is to create a focal vault over an inclusion cyst on the conjunctiva.5 Because a single area of modification would be made, any sized lens can be modified. This option is best for a lens that has a toric haptic or landing zone and is, therefore, non-rotational. When creating the focal vault or micro vault, the dimensions of the obstacle, an estimate of the height, and photographs of the lens on the eye are necessary. Specified measurements required to make this modification include the axis of the impediment, the distance of the impediment from the center of the lens, and the desired width of the focal vault. Because we are using the axis to specify a position, rather than a meridian, it is important to note that it must be specified from 0º to 360º, with 0º at 3 o’clock and the axis value increasing counterclockwise. For example, an inclusion cyst located at 6 o’clock would be specified as at 270º. The laboratory making the modification uses this information to remove part of the lens material sitting just above the obstacle.
Vaulting single focal areas, or multiple areas, inside the edge of the lens can also be accomplished with reverse geometry lens designs. By using a concentric lens curvature that scoops up between the haptic zone and the more central zone, it makes it possible to give added height over a circular lens zone. This lens design makes it possible to have a circular vaulting area that can be moved closer to, or farther from, the center of the lens. Because this zone is consistent in a circular pattern surrounding the center of the lens, this type of vaulting does not require a non-rotational lens and works well for both toric and spherical landing zones. More importantly, this design also allows a circular zone surrounding the central lens to be elevated in the midperiphery or paralimbal regions while keeping the central vault unchanged. This type of modification can be utilized in different ways depending on the obstacles present. For example, patients who have pellucid marginal degeneration and Salzmann’s nodular degeneration benefit reverse geometry closer to the edge. Post-penetrating-keratoplasty patients may require reverse geometry closer to the central zone (paracentral zone), and the circular nature of this extra vaulting can make it attractive when fitting over intracorneal ring segments.
BENEFITS AND CHALLENGES OF FITTING A LARGER-DIAMETER LENS
One basic, and perhaps most obvious, method to avoid scleral obstacles is to use a larger-diameter lens to vault over them completely. While larger-diameter lenses are great problem solvers, increasing the size of a lens can create additional challenges. The sclera itself often has more toricity compared with the cornea, and scleral toricity can increase farther from the cornea. Figure 3 shows scleral topography of an eye with little to no toricity in the sclera compared with an eye with considerable toricity of the sclera.
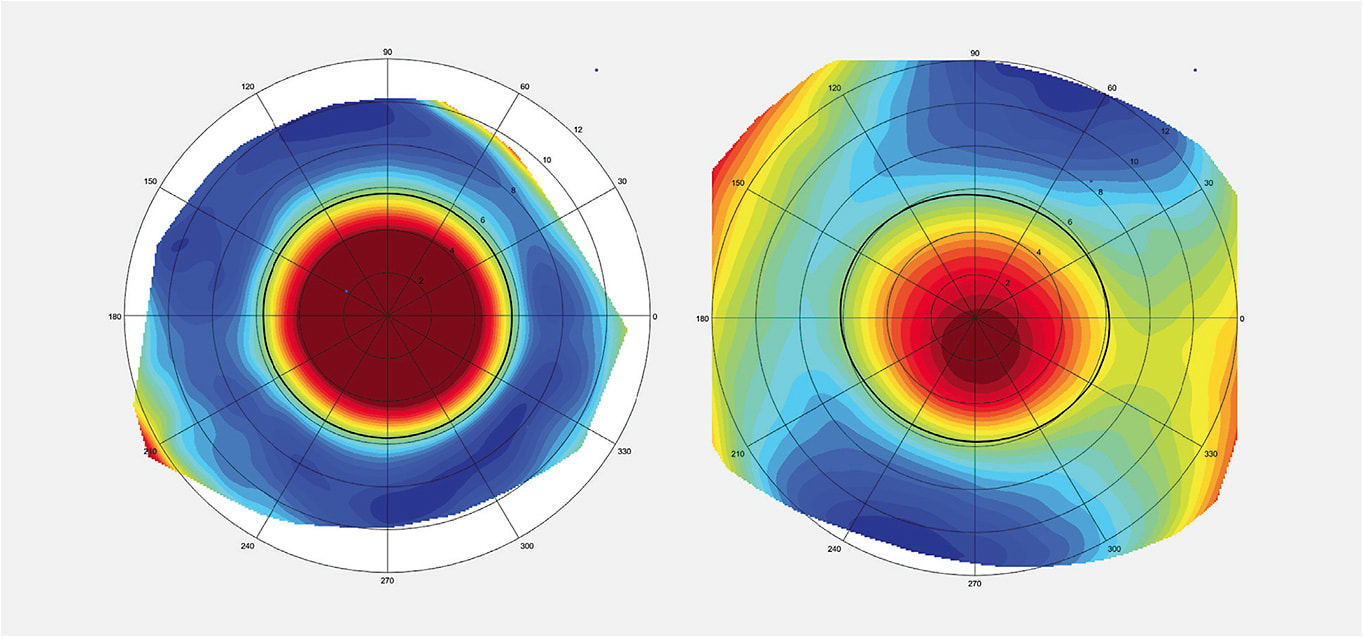
If fitting a scleral lens with a corneal topographer and a smaller-diameter diagnostic set, simply ordering the same lens with a larger diameter may result in unexpected lens fitting characteristics when it arrives. It is best to have diagnostic lens sets in varied diameters and to try larger lenses on the eye to assess what factors may be involved in fitting the most appropriately sized lens. Due to the greater possibility of toricity farther from the limbus, larger lenses are more likely to require special attention at the haptic zone. Many lens designs are available that can be customized to fit this scleral surface.
Adding Toricity to a Scleral Lens Fitting the haptic portion of the lens to match the contour of the sclera is important for fit and comfort regardless of the lens diameter. A lens that fits too tightly—whether in all portions of the lens or at one specific portion of the haptic—can cause pain and rebound redness when it is removed. Lenses that are fit too loosely tend to move excessively, causing discomfort and, at times, a “pumping” of air or debris under the lens with blinking. In many patients, using a diagnostic lens with a spherical haptic zone will result in both tight areas and loose areas at different portions of the eye. Adding toricity to the haptic of the lens can greatly improve the fit for these patients.
Fitting a scleral lens with a toric haptic zone has many benefits. While also improving the edge fit, a lens with different steep and flat meridians will not rotate freely on the eye. A non-rotational lens has greater stability for focal vaulting changes and for adding optical corrections such as front-surface toricity to correct residual astigmatism, multifocal components, or decentered optics to induce prism. In addition, utilizing a bitoric haptic can help improve the centration of a decentered lens.6
Assessing the haptic edge all the way around a lens can help determine whether it is appropriate to make the landing zone toric. When evaluating the edges of a diagnostic lens, the presence of blanching in one meridian is usually easily managed with a bitoric haptic. One method for visualizing the lens edge when assessing fit is to think of a cross section of the landing zone as if the entire haptic is a “foot.” Imagine that the toe of the foot is the very edge of the lens while the heel is at the inner boundary of the haptic. At times, blanching of vessels may occur at the very edge of the lens, which means the haptic is “toe down.” If blanching occurs inward, but not at the very edge, the haptic is “toe up,” with the “heel” pressing into the sclera.
Using the slit lamp beam to carefully examine the haptic 360º around the lens can help determine whether using a bitoric haptic is needed. The amount of change between the flattest and steepest meridian may also need to be increased or decreased depending on the differences in the edge fit. Many lens designs have stepwise degrees of toricity that can be ordered based on the appearance of the edge. In addition to blanching of vessels, it is possible to also assess differential edge lift with a slit lamp beam and high magnification. If an edge casts a shadow on the sclera with the beam oriented from the center of the lens toward the edge, the edge is toe up. To bring an edge down when it is toe up, the edge must be steepened. Wherever the lens edge is toe down and pressing into the sclera, an adjustment must be made to make that portion of the edge flatter to bring the toe upward.
Quadrant-Specific Customization of Scleral Lens Haptics At times, the edge lift around the perimeter of the lens appears to differ in positions that are not 90º apart but are instead seemingly inconsistent around the lens. Designs are now available that allow for quadrant-specific changes to the landing zone. Scrutinizing the edge 360º around the eye and making changes to the lift in every quadrant so that the haptic portion of the lens rests consistently on the sclera can improve both comfort and fit for these patients. Lens designs with this feature generally have fitting guides that assist in modifying the lenses. Online guides can help to visualize the changes needed as well, which can be helpful in evaluating a lens profile even after the patient has left the office.
BEYOND SLIT LAMP OBSERVATIONS: TECHNOLOGY CAN AID IN MAPPING SCLERAL CONTOUR
Scleral lens fitting can be successfully accomplished by using diagnostic lenses, carefully assessing clearance under the lens and alignment of the lens haptic, and then adjusting based on these observations. This process requires some amount of trial and error. Technology is available that can help in this process, whether to gain insight into a difficult fit or to assist in obtaining measurements before beginning a new fit.
Fluorescein-Based Scleral Topography Technology is available that utilizes fluorescein and wide-angle mapping to help troubleshoot lens fits. Utilizing a diagnostic lens in conjunction with scleral topography can make fitting extremely accurate and can decrease the amount of reorders needed. These instruments can be used to visualize the contour of the scleral lens and are generally associated with specific lens designs.
In much the same way that corneal topography can provide greater insight into how to best fit a corneal GP lens, scleral topography can provide many more hints for fitting a scleral lens beyond what can be gained from corneal keratometry. Whether troubleshooting a diagnostic lens that does not fit the scleral contour adequately or deciding to base an initial fit on scleral topography, utilizing a fluorescein-based scleral topography instrument can help eliminate some of the trial and error involved in determining ideal sagittal lens depth and landing zone curves. Both of the scleral topography instruments currently available rely on fluorescein instillation into the eye before imaging; one utilizes dual fringe projection to take a single image, and the other uses scanning in multiple gazes, with software used to create a single resulting image.7,8 Both of these instruments are associated with laboratories and/or particular lens designs and have the ability to match lens contours to the scleral contours mapped by the imaging. Not only can these instruments help determine the haptic curvatures needed for a successful fit, but they can also help to digitally design a lens to vault over areas such as a filtering bleb or pinguecula (Figure 4).
When using scleral topography to assist in fitting a lens, it is still important to use a diagnostic lens to determine the prescription needed. Once the lens settles on the eye, an over-refraction should be obtained. Combining information gained from the fit of the diagnostic lens or the base curve of a patient’s current scleral lens with the over-refraction and scleral topography allows practitioners to work out the parameters of the lens to be ordered.
ANTERIOR SEGMENT TOMOGRAPHY
Scheimpflug imaging is useful in analyzing ocular contour for assessing corneal and scleral curvature. Instrumentation that includes this technology is commonly used in ophthalmology practices for assessment before various ocular surgeries, making it an easily accessible tool for scleral lens fitters who practice in a surgical ophthalmic office. Scheimpflug imaging is a type of photography that captures multiple cross sections at various angles to compile a three-dimensional representation of all anterior segment structures.9 An anterior eye segment tomographer, which uses this type of imaging, has the ability to map the surface of the eye and does not require fluorescein while capturing data. Recently, one such device has offered additional software specifically for fitting scleral lenses, with many different lens designs and laboratories included in the library of its fitting software.
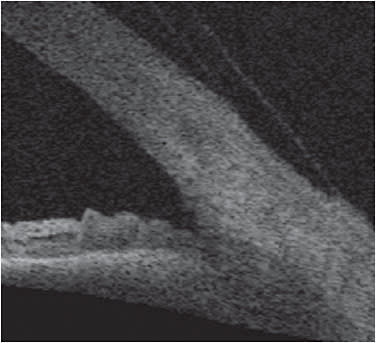
Optical coherence tomography (OCT) is also a great tool that can help evaluate clearance and edge alignment. OCT assessments of the anterior surface can be performed using a dedicated anterior segment OCT or an OCT that allows assessment of the posterior or anterior segment. While the cross-sectional images of the ocular surface are useful for estimating the sagittal depth of the eye, OCT instruments also allow practitioners to capture an image while a scleral lens is on the eye. Assessing clearance between the posterior surface of the scleral lens and the ocular surface can be performed by using calipers in the imaging software. Evaluating the toe up or toe down qualities of the scleral lens is easy when the edge of the lens is captured in the images (Figure 5). This is particularly useful when variations in edge lift are visible in different quadrants, making clear where a lens is not fitting the scleral contour well and modifications are needed. For example, it is easy to see a lens edge that is too steep, as it compresses the sclera. Ordering a flatter edge in the meridians in which this occurs can make a lens more comfortable for a patient.
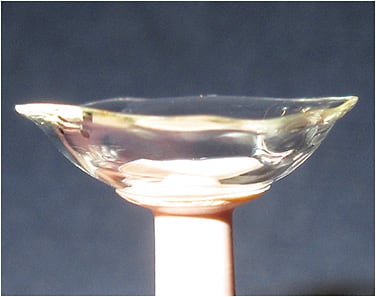
Impression-Based Fitting Impression-based fitting is an additional method of fitting scleral lenses that is particularly useful with irregularly contoured ocular surfaces. Whether the surface is irregular due to disease, scarring, or obstacles (e.g., cysts or blebs) maintaining consistent clearance over an irregular surface can be achieved by making an impression of the ocular surface to create a prosthetic device that perfectly matches the shape of that ocular surface. This method requires training from the manufacturer before becoming an approved practitioner. To create a lens, an impression of the ocular surface is first made in the office (Figure 6), and this impression is sent to the manufacturer where a 3D scanning process is used to create a scleral shell. Because the process is digital after the scan, duplicate lenses can later be made without repeating the impression step, assuming that the ocular surface has not changed in contour.

CONCLUSION
Scleral lens designs are becoming increasingly sophisticated as the use of these lenses increases. Knowing the options available and being able to assess the relationship between the ocular surface and a scleral lens can guide practitioners to create increasingly customized lenses. The use of diagnostic lenses is important, and slit lamp examination is critical to assess both the lens fit and the ocular health. In addition, technology is available to help refine the fitting process, with much help from laboratories in combining the clinical expertise of practitioners with the digital measurements that are now obtainable.
For references, please visit www.clspectrum.com/references and click on document #293.
CONTINUING EDUCATION CREDIT
Please take the post test by logging in at clspectrumce.com