



The inaugural Global Myopia Symposium (GMS) was hosted by the GMS Planning Committee—comprised of Chair Jason Nichols, OD, MPH, PhD; Kate Gifford, BAppSc(Optom)Hons; Lyndon Jones, PhD, DSc, FCOptom; Jeff Walline, OD, PhD; and myself—on Sept. 25 and 26 2020. What a year to launch a new meeting!
The original plan was to host a one-day meeting just prior to the well-established Global Specialty Lens Symposium in January 2021. But with each conference in 2020 slowly being cancelled, we decided to host the GMS meeting on its own, in a virtual format, and over two days in September. This turned out to be a blessing in disguise. The online format allowed more than 1,000 registrants to participate from more than 60 countries. Eyecare professionals, thousands of miles apart, were asking questions of each other, collaborating, and sharing ideas. Many of our speakers and attendees were active on all social media platforms, sharing their home set ups and revealing the secrets of their on-screen wardrobes. It was an empowering event.
Twenty internationally known speakers provided a total of 12 hours of education. Ten COPE-approved courses were offered for continuing education credits, including four general sessions and six breakout sessions. Attendees could earn up to eight live CE credits. Additionally, there were four sponsored talks that were packed with great information. A total of 13 industry partners came together to support this meeting.
Dr. Nichols initiated the symposium with a reminder of why we all chose to participate in this meeting and what working together could mean for the future of our children around the world. Dr. Walline encouraged all of us to be active listeners and to find six take-home messages that resonated with us—three of which we should start immediately upon returning to our clinical settings and three to work toward in the coming months. The biggest challenge was narrowing down the options to just six!
THE MARKETPLACE
Throughout the comprehensive two-day GMS program, five hours of dedicated time was set aside for attendees to visit the sponsor marketplace. They were encouraged to engage with the sponsors during this time, as each exhibitor had live representatives present to speak directly with attendees and to answer questions.
On the GMS platform, the sponsor marketplace was designed to allow our industry partners a space to provide resources including documents, videos, and handouts that could all be downloaded for future use in practice or on social media streams. Attendees could also request information by email.
THE BASICS: UPDATED
One message that many speakers repeated throughout the meeting was that more than half of the world’s population will be myopic by the year 2050, with an impact on the world’s economy of about $1.2 trillion. The primary concern with myopia is the risk of future complications. We know that retinal detachments, cataracts, and glaucoma are among these complications, but myopic macular degeneration (MMD) may pose the greatest threat to vision. Mark Bullimore, MCOptom, PhD, noted that low amounts of myopia do not eliminate the risk; there is no safe level of myopia, as one-half of those who have MMD have low myopia. By 2050, not only will about half of the world be myopic, 55.7 million will suffer from MMD, and 18.7 million will be blind.
MMD was noted to be the only leading cause of blindness that does not have an established treatment. This is the reason why we all need to fight myopia. Dr. Bullimore showed us that by controlling just 1.00D of myopia, we reduce the risk of MMD by 40%.
How do we predict future progression of myopia? We can no longer look at the past progression of a child’s myopia. Year one does not indicate what will occur in year two. We know that the younger the age of onset, the greater the overall progression will be. But, we also know that the absolute refractive treatment effect is constant regardless of age, race, or progression rate. Therefore, we must look at axial length along with refractive error to help us predict future levels of myopia, using our best judgment until we have growth curves available to guide us more effectively.
We also learned that most of the treatment effect occurs in the first year of myopia management. Year two and three combined will still not equal year one’s reduction. This is all relevant so that we can better educate our parents and also better understand the path of myopia progression.
Axial elongation will become the gold standard for tracking myopia progression, assessing risk of myopia, and predicting future amounts of myopia. Axial elongation is easier to measure. It is more accurate and consistent, it is independent of changes to the eye such as those with orthokeratology and atropine use, and patients do not need to undergo a cycloplegic refraction to be monitored.
OCULAR RISKS—CORNEAL OR RETINAL
Any amount of myopia comes with risk. Figure 1 shows the amount of risk based on myopic refractive error.1-4 Figure 25 shows the risk based on axial length at both age 60 and 75.


Dr. Kate Gifford presented data on the risk of microbial keratitis (MK) with contact lens wear versus visual impairment. She compared two children who had the same prescription, the same age, and the same one-year rate of progression. One child’s family chose conventional eyeglasses, and the other child’s family chose myopia management with orthokeratology They were evaluated throughout their lives at various ages while their level of myopia and associated risk of MK and visual impairment were outlined. The visual representations were quite compelling in demonstrating the higher risk of visual impairment with a higher level of myopia, whereas one decision years ago put the second child in a much lower risk category for visual stress (Figure 3).

TREATMENT OPTIONS
Optical Treatments Simplified Paul Gifford, PhD, MCOptom, discussed optical myopia management treatment options and how they actually work. He demonstrated, using very simple diagrams, the optics of uncorrected myopia, corrected myopia, and myopia management treatment options. The ray drawings helped to visualize the impact of peripheral rays focused behind the retina and how axial elongation occurs as a result. Spherical aberration and depth of focus were equally well explained.
Percentage Efficacy of Treatment Options Understanding the limitations of using percentages of efficacy, Dr. Kate Gifford provided a simple diagram that looked like an awards podium to help group the treatments for the purpose of guiding our patients. The best options were in the gold or first-place position (~50%) on the podium and included orthokeratology, the dual focus multifocal soft lens, and the defocus incorporated multiple segments (DIMS) ophthalmic lens. The silver podium position (~33%) included a center-distance soft multifocal lens with a +2.50D add, bifocal ophthalmic lenses, and bifocal and prismatic ophthalmic lenses. The treatment options in the bronze position (minimal impact) are progressive and peripheral defocus ophthalmic lenses. Atropine concentrations can also be placed on a similar podium, with 0.05% in the gold position (~50%), 0.025 in the silver position (~33%), and 0.01% in the bronze position (minimal impact).
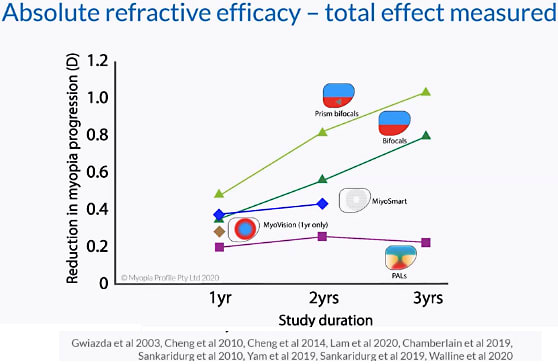
Defining Efficacy Dr. Bullimore noted that we need to change the way in which we discuss efficacy of myopia treatment options and the goals for patients. It was emphasized that we need to stop discussing the efficacy in terms of percentages and talk about it more in terms of millimeters (mm) and diopters (D).
Dr. Kate Gifford summarized absolute refractive efficacy in diopters and absolute axial length efficacy in millimeters in two simple charts demonstrating the impact of reducing myopia over each of three years (Figures 4 and 5). Based on data by Hu et al, what we know is that earlier onset of myopia leads to higher levels of myopia.6 In addition, we know that the absolute refractive efficacy is constant with age, race, and progression rates. We also know that progression of refractive error and of axial elongation slows as children age. Dr. Gifford noted that race does impact axial elongation, with Asians elongating 40% faster compared to non-Asians. What practitioners need now are growth curves to help us determine an individual’s progression rate.

When looking at studies and using the cumulate absolution reduction in elongation (CARE) method of analyzing data, Dr. Bullimore indicated that we can see that there is only 1.20D of refractive error reduction in myopia progression and 0.44mm of axial length reduction. This information changes so much of what we believe as well as how we have been assessing treatment options and counseling parents.
OCULAR COMPLICATIONS
Jessica Haynes, OD, did a wonderful job outlining the ocular complications of myopia that impact the retina. She explained layer by corneal layer the various complications that myopia can cause. She noted that common findings include tilted disc, tesselated fundus, posterior staphyloma, thin choroid, macular degenerations, peripheral retina degenerations, and vitreoretinal interface disease.
Dr. Haynes reviewed protocols for treatment and follow-up schedules. She indicated that posterior staphylomas are the hallmark of pathological myopia and represent an area of research that we will be hearing more about in the future.
IMPLEMENTATION IN PRACTICE
Many facets must be considered when introducing myopia management into practice, and the GMS presenters tackled many of these issues and provided helpful tips and advice. Some of the important messages that were shared by many speakers included:
- Great communication with patients and their parents is both needed and important.
- Practitioners need to have resources available to explain their processes and defend their claims. We communicate the important information, but patients may hear very little. They need information that they can absorb at home.
- Practitioners need to involve staff to help with patient/parent conversations to reduce chair time.
- The parents and children in our myopia management programs are our best marketers.
- Fees are complicated—but necessary—and practitioners cannot sell themselves short.
Gary Gerber, OD, discussed a systematic approach to implementing myopia management into our practices. He encouraged audience members to commit fully to myopia management rather than being just a “myopia dabbler.” Staff engagement is a top priority for him; making sure that each team member understands and is committed to the underlying goal is crucial to establishing a fully operational myopia management clinic.
Alan Glazier, OD, discussed the components of an initial examination, the follow-up tests, and the frequency of follow-up visits in years one and two of treatment. He discussed U.S. Food and Drug Administration approvals and informed consent as well as the need to be realistic and to not over-promise parents.
Stephanie Ramdass, OD, MS, MBA, discussed fee structures, bundles, and packages. She also explained how to adapt to parental or patient hesitations, concerns, and limitations such as costs and time.
Many cases were presented by various speakers over the two days, and the questions that attendees asked most revolved around how to make clinical decisions to follow, change, or add to a treatment regimen. Tracking and benchmarking a patient’s progression is accomplished through repeated measurements of both axial length and cycloplegic refractive error. Dr. Glazier reminded us that we cannot stop progression; we will still see change, we can only slow myopia down. The average rate of change annually is 0.2mm in axial length growth and 0.50D of myopia increase. If that can be reduced by half, then we are reducing a patient’s progression. As discussed by Dr. Kate Gifford and Dr. Bullimore, efficacy and amount of change are under investigation; growth, axial length, and refractive error charts relative to age and race are being developed that will help us make better clinical decisions in the future.
The marketing strategies presented by Jason Compton, OD, were very popular. He noted the need to increase patient awareness internally followed by external marketing. Drip campaigns, marketing materials in our office waiting rooms, and external marketing were all discussed, including the difference between intent marketing online and distraction marketing via social media.
THE EMOTIONS OF MYOPIA
Karen Walsh, BSc(Hons), PGDip, MCOptom, explored the social, emotional, and psychological aspect of myopia from the viewpoint of having been a myopic child and of now being a parent of a myopic child and an eyecare professional treating myopia. She shared the isolation that she felt and the impact on her self-esteem and on her confidence as a myopic teenager. She explained that her engagement and performance in sports were hindered. As a parent of a myopic child, she shared her guilt, her concerns and questions, and the struggles faced at home with her son going through an orthokeratology fitting.
Being able to empathize and understand our patients and their parents will help practitioners better understand what our value proposition is. Myopia management needs to evoke an emotion with parents. They need to feel what it is that we can do to help their child: improve their vision, their ability to learn in school, their performance in sports, their self esteem, their confidence, and their quality of life; expand their refractive surgical options later in life; and provide a future with less risk of ocular complications. The value is evident; we just need to know how best to communicate it.
BENEFITS FOR ALL
The GMS sessions provided so much information, and the comments and questions were engaging and thought-provoking. There was humor, debates, collaborations, networking, information shared, and much enjoyment while each of us were safe at home. And if you missed a session or couldn’t choose between the simultaneously held breakout sessions, all of the sessions are available on demand until Dec. 26, 2020.
From lemons, the best lemonade was made. For two days, we were immersed with colleagues from around the world, learning, collaborating, and pushing a common agenda forward. The energy was contagious, and I walked away feeling invigorated and charged to do more. In the chaos of 2020, the one thing that we have learned is that we are all in this together working on a common goal to rid the world of myopia. The only way to push forward is together, with more research, more education, and continuing to support and push each other. We look forward to coming together again at the next GMS. CLS
REFERENCES
- Younan C, Mitchell P, Cumming RG, Rochtchina E, Wang JJ. Myopia and incident cataract and cataract surgery: the blue mountains eye study. Invest Ophthalmol Vis Sci. 2002 Dec;43:3625-3632.
- Ogawa A, Tanaka M. The relationship between refractive errors and retinal detachment--analysis of 1,166 retinal detachment cases. Jpn J Ophthalmol. 1988;32:310-315.
- Vongphanit J, MItchell P, Wang JJ. Prevalence and progression of myopic retinopathy in an older population. Ophthalmology. 2002 Apr;109:704-711.
- Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012 Nov;31:622-660.
- Tideman JW, Snabel MCC, Tedja MS. Association of Axial Length With Risk of Uncorrectable Visual Impairment for Europeans With Myopia. JAMA Ophthalmol. 2016 Dec 1;134:1355-1363.
- Hu Y, Ding X, Guo X, Chen Y, Zhang J, He M. Association of Age at Myopia Onset With Risk of High Myopia in Adulthood in a 12-Year Follow-up of a Chinese Cohort. JAMA Ophthalmol. 2020 Sept 17;e203541.
Figure 4 References
- Gwiazda J, Hyman L, Hussein M, et al. A ramdomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Opthalmol Vis Sci. 2003 Apr;44:1492-1500.
- Cheng D, Schmid KL, Woo GC, Drobe B. Randomized trial of effect of bifocal and prismatic bifocal spectacles on myopic progression: two-year results. Arch Ophthalmol. 2010 Jan;128:12-19.
- Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014 Mar;132:258-264.
- Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomized clinical trial. Br J Ophthalmol. 2020 Mar;104:363-368.
- Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical trial of MiSight Lenses for Myopia Control. Optom Vis Sci. 2019 Aug;96:556-567.
- Sankaridurg P, Donovan L, Varnas S, et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optom Vis Sci. 2010 Sep;87:631-641.
- Yam JC, Jiang Y, Tang SM, et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology. 2019 Jan;126:113-124.
- Sankaridurg P, Bakaraju RC, Naduvilath T, et al. Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomized clinical trial. Ophthalmic Physiol Opt. 2019 Jul;39:294-307.
- Walline JJ, Walker MK, Mutti DO, et al. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA. 2020 Aug 11;324:571-580.
Figure 5 References
- Gwiazda J, Hyman L, Hussein M, et al. A ramdomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Opthalmol Vis Sci. 2003 Apr;44:1492-1500.
- Cheng D, Schmid KL, Woo GC, Drobe B. Randomized trial of effect of bifocal and prismatic bifocal spectacles on myopic progression: two-year results. Arch Ophthalmol. 2010 Jan;128:12-19.
- Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014 Mar;132:258-264.
- Sun Y, Xu F, Zhang T, et al. Orthokeratology to control myopia progression: a meta-analysis. PLoS One. 2015 Apr 9;10:e0124535.
- Si JK, Tang K, Bi HS, Guo DD, Guo JG, Wang XR. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015 Mar;92:252-257.
- Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomized clinical trial. Br J Ophthalmol. 2020 Mar;104:363-368.
- Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical trial of MiSight Lenses for Myopia Control. Optom Vis Sci. 2019 Aug;96:556-567.
- Sankaridurg P, Donovan L, Varnas S, et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optom Vis Sci. 2010 Sep;87:631-641.
- Sankaridurg P, Bakaraju RC, Naduvilath T, et al. Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomized clinical trial. Ophthalmic Physiol Opt. 2019 Jul;39:294-307.
- Yam JC, Jiang Y, Tang SM, et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology. 2019 Jan;126:113-124.
- Walline JJ, Walker MK, Mutti DO, et al. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA. 2020 Aug 11;324:571-580.