


EDITED BY CHAD ROSEN, OD, MBA
This course is COPE approved for 2 hours of CE credit and NCLE General Knowledge approved for 2 hours of CE credit.
COPE Course ID: 68074-CL NCLE Course ID: CWCLS003
Release Date: July 1, 2020 Expiration Date: June 2, 2023

LEARNING METHOD AND MEDIUM
This educational activity consists of a written article and 20 study questions. The participant should, in order, read the Activity Description listed at the beginning of this activity, read the material, and answer all questions in the post test.
To receive credit for this activity, please follow the instructions provided below in the section titled To Obtain CE Credit. This educational activity should take a maximum of 2 hours to complete.
CONTENT SOURCE
This continuing education (CE) activity captures key statistics and insights from contributing faculty.
ACTIVITY DESCRIPTION
The goal of this article is to better eyecare professionals’ understanding of scleral lenses for therapeutic use for dry eye and ocular surface disease.
TARGET AUDIENCE
This educational activity is intended for optometrists, contact lens specialists, and other eyecare professionals.
ACCREDITATION DESIGNATION STATEMENT
This course is COPE approved for 2 hours of CE credit and NCLE General Knowledge approved for 2 hours of CE credit.
COPE Course ID: 68074-CL
NCLE Course ID: CWCLS003
DISCLOSURES
Kate A. McClure, OD, MS, has received honorarium from Contamac, Euclid, and Valley Contax.
Chad Rosen, OD, MBA, editor of the continuing education series, reports no conflicts of interest.
DISCLOSURE ATTESTATION
The contributing faculty member has attested to the following:
- That the relationships/affiliations noted will not bias or otherwise influence her involvement in this activity;
- That practice recommendations given relevant to the companies with whom she has relationships/affiliations will be supported by the best available evidence or, absent evidence, will be consistent with generally accepted medical practice;
- That all reasonable clinical alternatives will be discussed when making recommendations.
TO OBTAIN CE CREDIT
To obtain COPE CE credit for this activity, read the material in its entirety and consult referenced sources as necessary. We offer instant certificate processing for COPE credit. Please take the post test and evaluation online by using your OE tracker number and logging in to clspectrumce.com .
Upon passing the test, you will immediately receive a printable PDF version of your course certificate for COPE credit. On the last day of the month, all course results will be forwarded to ARBO with your OE tracker number, and your records will be updated. You must score 70% or higher to receive credit for this activity. Please make sure you take the online post test on a device that has printing capabilities.
To obtain NCLE credit, a score of 80% or higher is required. Passing scores will be forwarded to ABO-NCLE at the end of each month.
NO-FEE CONTINUING EDUCATION
There are no fees for participating in and receiving credit for this activity.
DISCLAIMER
The views and opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of NOVA Southeastern University College of Optometry or Contact Lens Spectrum. This CE activity is copyrighted to PentaVision LLC ©2020. All rights reserved.
This continuing education activity is supported by unrestricted grants from ABB Optical Group, Blanchard Contact Lenses, BostonSight, Menicon, and X-Cel Specialty Contacts.
RELEASE DATE: JULY 1, 2020
EXPIRATION DATE: JUNE 2, 2023
To view this CE activity in its entirety and proceed to the test, visit clspectrumce.com
Dry eye disease (DED) is a multifactorial disease that disrupts the tear film and causes ocular surface inflammation. In moderate-to-severe or refractory DED, scleral lenses can improve signs and symptoms by maintaining ocular surface hydration. They are used when traditional treatments have failed, but before surgical intervention. Additionally, patients who have severe ocular surface disease (OSD) can benefit from the protection and constant lubrication provided by scleral lenses. This article will focus on their therapeutic use for dry eye and OSD.
DRY EYE DISEASE CLASSIFICATIONS
Although many patients suffer from DED, the reported prevalence ranges from 5% to 50% due to challenges in standardizing the diagnostic criteria.1 DED has two predominant etiologies—aqueous deficient and evaporative—though they are not mutually exclusive and often exist on a continuum.2 Conditions that affect the eyelids and ocular surface are classified as evaporative DED, including blink abnormalities and meibomian gland dysfunction—the leading cause of DED.1 Aqueous deficient DED, however, is caused by inadequate tear volume due to an insufficiency in lacrimal gland secretion. Aqueous deficient DED can further subdivide into Sjögren’s and non-Sjögren’s lacrimal gland disease.
Non-Sjögren’s Aqueous Deficient DED Non-Sjögren’s aqueous deficient DED is caused by a decrease in function of the lacrimal gland, largely attributed to aging hormonal changes. Other contributing factors include a decrease in sensation from the ocular surface, secretory neurotransmitters, and functional secretory tissue.3 Non-Sjögren’s DED progresses more slowly and is often less severe when compared with Sjögren’s DED.
Sjögren’s Aqueous Deficient DED Chronic Sjögren’s is an autoimmune disease of exocrine gland dysfunction that targets the salivary and lacrimal glands. Sjögren’s DED damages the lacrimal gland by infiltration of lymphocytes and other immune cells.3 Incidence of diagnosed Sjögren’s among Caucasians in the U.S. is 3.9 per 100,000 per year, with a rate 14 times higher in women.4 Secondary Sjögren’s is a systemic autoimmune disorder that co-exists with rheumatoid arthritis, systemic lupus erythematosus, or Wegener’s granulomatosis. Approximately 26% of patients who have aqueous deficient or evaporative DED have a rheumatological condition, and 10% of patients who have aqueous deficient DED have Sjögren’s.5,6 Any patient who has a rheumatological condition must be evaluated closely for signs and symptoms of DED.
SCLERAL LENSES FOR DRY EYE DISEASE TREATMENT
The 2017 TFOS DEWS II Report provides a staged treatment algorithm for DED. It is recommended that practitioners do not follow the algorithm in a rigid, stepwise approach, but rather use the recommendations as a guideline to provide evidence-based treatment. The treatments are summarized in Table 1.
| STAGE 1 |
|
| STAGE 2 |
|
| STAGE 3 |
|
| STAGE 4 |
|
Scleral lenses are a treatment consideration for moderate-to-severe or refractory DED. Scleral lenses can be used therapeutically to treat DED, specifically aqueous deficient lacrimal gland dysfunction when ocular surface staining is present. The fluid reservoir bathes the ocular surface, providing constant hydration and lubrication.8 Therapeutic scleral lens wear can be particularly beneficial for patients who have Sjögren’s and rheumatological conditions, due to the severity of the DED. The lenses can help stabilize the tear film, break the cycle of ocular surface inflammation, and restore homeostasis.9
Therapeutic contact lenses are incorporated into Step 3 of the TFOS DEWS II treatment algorithm and should not be used as first-line therapy. Scleral lenses should be reserved for the management of DED when other therapies have failed to provide adequate treatment but before surgical intervention is considered (Figure 1).7,9,10
SCLERAL LENSES FOR OCULAR SURFACE DISEASE
There are numerous therapeutic indications for scleral lens wear in the treatment of OSD. Therapeutic OSD indications for scleral lens wear include Stevens-Johnson syndrome, chronic graft-versus-host disease (GVHD), ocular cicatricial pemphigoid (OCP), Sjögren’s, persistent epithelial defect (PED), limbal stem cell deficiency, superior limbic keratoconjunctivitis, exposure keratopathy, neurotrophic keratitis, trichiasis, and entropion.11-13
Graft-Versus-Host Disease GVHD is an immune-mediated, inflammatory disorder that can result after allogenic hematopoietic stem cell transplantation. Many organs and tissues can be targeted, including the ocular surface. Advanced DED is the most common ocular manifestation, leading to severe meibomian glands dysfunction and destruction of the lacrimal gland by allogenic T-cells.14 In addition to lacrimal gland destruction, the cornea, conjunctiva, and eyelids can be affected, ultimately leading to corneal scarring and symblepharon formation.3 Scleral lenses can improve ocular symptoms and reduce the Ocular Surface Disease Index (OSDI) score in patients with GVHD.15 The lenses improve the integrity of the ocular surface in GVHD by reducing ocular surface staining, epithelial defects, and filamentary keratitis.15
Mucous Membrane Pemphigoid This disease is a severe chronic autoimmune blistering condition that affects mucous membranes of the body and ocular surface. OCP refers to the condition when the ocular conjunctiva is affected. In OCP, meibomian gland duct obstruction occurs, resulting in severe dry eye. The blistering can lead to a shortening of the fornix and to formation of a symblepharon and ankyloblepharon. An entropion and trichiasis can result, causing corneal neovascularization and scarring.3 Scleral lenses provide protection to the ocular surface and essential, constant lubrication in cases of OCP.
Stevens-Johnson Syndrome This condition is a life-threatening, acute blistering disease of the skin and mucous membranes. Stevens-Johnson syndrome is a T-cell mediated type IV hypersensitivity reaction often caused by medications, specifically antibiotics,3 and it can affect the cornea and conjunctiva by complete absence of tear production, leading to corneal and conjunctival scarring.16 Scleral lenses improve visual acuity and reduce photophobia in patients who have Stevens-Johnson syndrome, providing more relief than the topical lubricants, autologous serum drops, and corticosteroids that are often used.17
Persistent Epithelial Defect A persistent epithelial defect must be treated promptly and aggressively to prevent corneal ulceration, which can lead to corneal melt and perforation. Standard treatments include the use of topical medication, lubricants, cyclosporine, autologous serum tears, bandage contact lenses, and amniotic membranes. When other therapies fail, a fluid-ventilated GP scleral lens device may be used to repair the corneal surface.18
The recommended treatment protocol specifies extended wear of the scleral lens for a short duration, until there is complete re-epithelization of the persistent epithelial defect.18 The device is removed for brief cleaning and disinfecting during this extended wear period. The patient may need to wear the scleral lens device for 24 to 48 hours after re-epithelization to prevent reoccurrence. During this period of extended wear, a drop of BAK-free moxifloxacin 0.5% is placed in the bowl of the scleral lens, along with the nonpreserved saline, for prophylaxis to reduce the risk of microbial keratitis.18 Following resolution of the persistent epithelial defect, daily scleral lens wear should be initiated.
BENEFITS OF THERAPEUTIC SCLERAL LENSES
Scleral lenses for the treatment of moderate-to-severe DED and OSD are advantageous due to the protection that the fluid reservoir provides to the ocular surface. The lenses provide mechanical protection and heal the corneal and conjunctival surface with constant lubrication and moisture.
Patients who have OSD and severe DED often require frequent or constant lubrication, and scleral lenses can help reduce the number of drops used throughout the day.19 The reservoir prevents the dehydration of the ocular surface. The lenses can provide relief from symptoms of severe pain and photophobia by improving the integrity of the ocular surface.9
Scleral lens wear reduces ocular surface staining induced by OSD and DED. An improvement in the integrity of the ocular surface can be evaluated by assessing corneal and conjunctival staining prior to scleral lens wear and again after scleral lens treatment.19 The integrity of the ocular surface can be improved with therapeutic scleral lens wear, reducing ocular surface staining, and as a result, an improvement in visual acuity is often achieved.10
Scleral Lenses for Drug Delivery in OSD Corneal neovascularization can result from severe OSD, particularly in patients who have OCP, Stevens-Johnson syndrome, and GVHD. Corneal neovascularization can reduce visual acuity and promote corneal opacification. The presence of vascular endothelial growth factor (VEGF) causes neovascularization of the eye, and anti-VEGF therapies have become the first-line therapy in treating retinal vascular disease.
Application of the VEGF inhibitor bevacizumab to the ocular surface has been demonstrated to improve corneal neovascularization.20 Patients who have active or vision-threatening corneal neovascularization used one drop of 1% preservative-free bevacizumab, along with buffered nonpreserved saline, in a large-diameter, fluid-ventilated scleral lens. The treatment was found to be safe and significantly reduced the corneal neovascularizaiton.20
Further investigation is warranted to determine whether scleral lenses can be a drug delivery device for other ocular medications.
HYPOXIC RISKS WITH SCLERAL LENS WEAR
Risk versus benefit is a consideration for therapuetic scleral lens wear in both DED and OSD. Scleral lenses are considered to be a safe and effective treatment, with relatively low risks and mostly minor complications.8 However, hypoxic stress to the cornea should be a risk consideration. The goal is to prevent corneal swelling and complications secondary to hypoxia, including neovascularization.
Scleral lenses are manufactured in high-oxygen-permeable materials that have a Dk value of 100 or greater. The rate of hypoxic complications are low in scleral lens wearers, with 5% of patients developing corneal edema and 4% developing neovascularization.19 The levels of oxygen reaching the cornea are variable and are dependant on the lens material, the lens center thickness, and the thickness of the fluid reservoir.
There is an increased risk for corneal swelling when the saline reservior is greater than 250µm thick after settling.21 If a patient is at risk for hypoxia, the final clearance should be kept at a minimum, less than 250µm.
With the advent of newer hyper-Dk materials for scleral lenses, there are more options when hypoxia is a concern. Maintaining an appropriate lens center thickness is imperative but is dependant on various lens parameters, including the lens power, material, and overall lens diameter. Smaller-diameter lenses generally have a thinner center thickness. When the center thickness of the lens is a concern, a smaller-diameter scleral lens may be prefered over a large-diameter lens. It has been suggested that a maximum lens center thickness of 250µm may be indicated to prevent corneal swelling in patients who are at risk for hypoxia.21
STRATEGIES FOR FITTING SUCCESS
When fitting scleral lenses in patients who have OSD or DED, attention to lens diameter, corneal clearance, and the landing zone is key.
Scleral Lens Diameter The internationally accepted nomenclature, determined by the Scleral Lens Education Society, differentiates scleral lenses by their size relative to the horizontal visible iris diameter (HVID). All lenses that rest entirely on the sclera are considered scleral lenses. A mini-scleral is up to 6mm larger compared with the HVID, and a large-diameter scleral lens is 6mm greater compared with the HVID.22
Large-diameter scleral lenses are often used for DED and OSD to hydrate and protect more of the ocular surface. When indicated, a smaller mini-scleral lens can provide therapeutic benefits.11 The center thickness is generally thinner in a smaller-diameter lens, which can be advantageous for allowing more oxygen to the cornea. Mini-scleral lenses can be easier for handling and application, which is beneficial for patients who have smaller apertures or shortened fornixes secondary to OSD.
Central and Limbal Corneal Clearance The sagittal depth of the scleral lens vaults over the corneal surface, creating the fluid reservoir. The depth of this reservoir is referred to as the clearance. The clearance is minimized as the lenses are worn, termed settling, and is patient dependent. Most scleral lenses settle 100µm to 150µm. After 4 hours of wear time, approximately 80% of the settling has occurred.23 The goal is to achieve a final central clearance of 150µm to 250µm, but 50µm to 100µm may be adequate in some cases.24
Less central clearance is needed to vault a normal corneal curvature due to the more uniform shape. Patients who have OSD and irregular corneas may require a greater central clearance. The lens must appropriately vault the limbus, and typically 50µm to 100µm is sufficient to avoid complications.24
Once the lens is fully settled, it should be removed and the ocular surface should be evaluated for fluorescein staining. Corneal staining present at the limbus indicates insufficient limbal clearance.
Scleral Lens Landing Zone Proper alignment of the scleral lens landing zone is critical to achieve a successful fit. Smaller-diameter lenses—15mm or less—avoid the asymmetrical portion of the sclera, therefore a spherical landing zone can often be utilized.24 Larger-diameter lenses will often require a toric landing zone to achieve proper alignment and to avoid complications.
A lens that does not have proper alignment with the sclera may decenter, impacting the overall fit and compromising vision as a result of decentered optics.23 Sectoral or localized conjunctival blanching, impingement, and prolapse result when the lens does not align with the scleral toricity.24 Poor alignment may also stimulate debris accumulation in the saline reservoir, which will be further discussed.
There are various methods for assessing the scleral landing zone alignment. Using slit lamp evaluation, conjunctival blanching at the edge of the lens indicates that the respective meridian is too steep. Alternatively, if the edge is lifting off, the landing zone is too flat. Fluorescein can be instilled around the edge of the lens, and if the fluorescein influx is immediate and significant, the corresponding landing zone meridian should be steepened.
The use of anterior segment optical coherence tomography (OCT) imaging is useful for evaluating the scleral landing zone alignment.8 OCT may be used to image the lens edge in different positions of gaze to determine whether the lens edge is lifting off of or impinging the conjunctiva.
CHALLENGES AND COMPLICATIONS
Scleral lenses can provide many benefits to patients who have DED and OSD; however, there are common challenges that practitioners may encounter. Fogging caused by debris accumulation in the post-lens fluid reservoir can be problematic. Determining the source of the fogging is key to effectively treat and remedy the complication. DED and OSD patients are also prone to deposits on the lens surface.
Scleral Lens Surface Deposits Deposits on the scleral lens surface are common in patients who have DED and OSD, due to the poor quality of the tear film. Meibomian gland dysfunction is common in patients who have DED and OSD and is often the source of anterior lens surface deposits. Meibomian gland disease should be treated aggressively with warm compresses, lid hygiene, and more advanced treatments, if necessary. If mechanical removal of the deposits is indicated, the patient may remove the lens to clean the surface with GP contact lens solution prior to re-applying. This may not be ideal, as frequent application and removal of the lens may exacerbate the inflammatory response and mucin production. Alternatively, patients may use conditioning solution applied to a cotton-tipped applicator or to the edge of a plunger to mechanically remove the deposits while the lens remains on the eye.
A specialized polyethlene glycol-based surface coating may be added to the lens during the manufacturing process to help reduce deposits and promote better wettability of the lens surface. The coating can create a more comfortable wearing experience for patients. If deposits continue to accumulate, inquire about cosmetics, creams, or lotions that patients may be applying and incidentally transferring to the lens surface.
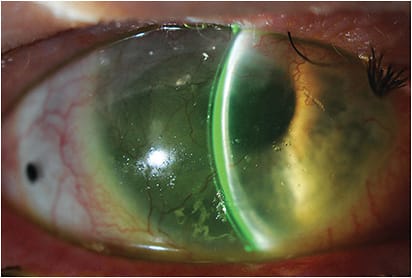
When surface deposits and non-wetting continue to be problematic (Figure 2), an alternative lens material or a different cleaning system may be required.
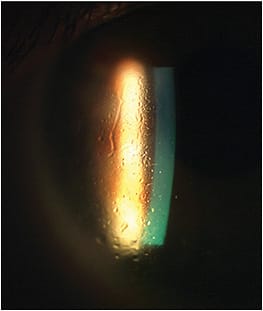
Debris in Fluid Reservoir Debris accumulation in the post-lens fluid reservoir creates fogging and can occur within minutes or hours of lens wear. When the fogging is significant, patients may be required to remove the lens, clean it, and fill it with fresh nonpreserved saline. As mentioned previously, frequent scleral lens removal may induce inflammation and mucin production, further exacerbating the fogging (Figure 3).

To prevent excessive debris in the reservoir, first ensure that the scleral lens fit is optimal. Excessive central or limbal clearance can lead to post-lens fogging. The scleral landing zone must be well-aligned with the sclera to prevent tear debris accumulation caused by excessive edge lift.
If the lens fit is optimal but ocular surface inflammation still induces tear debris, patients may insert several drops of a thick, preservative-free artificial tear into the bowl of the lens prior to filling the remainder of the bowl with preservative-free saline.11 This will increase the viscosity of the fluid and prevents debris accumulation in the fluid reservoir.
Modifying the type of non-preserved saline may be helpful. Nonpreserved saline is buffered to match the pH of the tears or is non-buffered. Patients who have DED and OSD may benefit from a buffered saline, which is less acidic. A new nonpreserved saline is available with electrolytes to mimic natural tears. This could be beneficial to potentially reduce ocular surface inflammation and complications of lens fogging.
CONCLUSION
Scleral lenses provide a safe and effective treatment for moderate-to-severe DED and OSD. The therapeutic use of scleral lenses has been well-established to improve signs and symptoms by restoring the integrity of the ocular surface.
Scleral lenses provide ocular surface protection and hydration necessary for many patients. As noted, achieving a successful fit is essential to prevent complications.
For references, please visit www.clspectrum.com/references and click on document #296.
CONTINUING EDUCATION CREDIT
Please take the post test by logging in at clspectrumce.com