



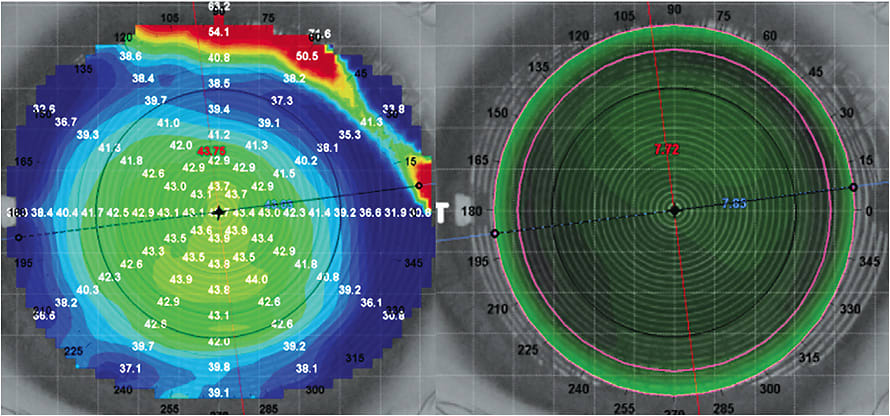
Empirical fitting methodology allows practitioners to supply a contact lens laboratory with minimal pre-fitting information, such as keratometry values and refraction, to generate an effective lens without having to place any diagnostic lenses on the eye. Current automated manufacturing lab equipment makes the success of empirical designs more likely in comparison to 10 to 20 years ago due to higher-quality lenses with newer edge designs. Likewise, modern topographical software programs allow practitioners to better measure ocular shape for creation of empirical and even virtually designed specialty lenses (Figure 1). For pediatric patients, empirical fitting decreases chair time by eliminating diagnostic lens fitting. This is both efficient and patient-friendly, especially in first-time wearers that may be nervous.
Empirical fitting also means that a new, unworn lens will be fitted to one patient only. If reusable lenses are not disinfected properly when used to perform a diagnostic lens fitting, there is potential for transferring harmful pathogens from one patient to another. Empirical fitting eliminates that risk by providing a lens to a patient that has never been worn.
If diagnostic lens fitting is necessary, disinfection following standards from the 2018 International Organization for Standardization 19979:2018(E) should be followed. The American Optometric Association’s Contact Lens & Cornea Section and The American Academy of Optometry’s Section on Cornea, Contact Lenses and Refractive Technologies has also created guidelines (2019) for practitioners to follow for proper diagnostic lens disinfection.
A Case in Point
Consider a 13-year-old male who has Down syndrome referred for contact lens fitting for his keratoconus. Retinoscopy revealed a scissoring reflex in both eyes, with a –16.00 –3.50 x 042 and –10.00 –7.00 x 162 prescription in the right and left eyes, respectively. Keratometry values were 55.70D @ 155 / 75.00D @ 065 OD and 50.06D @ 131 / 59.47D @ 041 OS. His mother was also concerned about him dislodging lenses during wear due to his habit of eye rubbing. A corneoscleral GP lens was determined to provide him with the best quality of vision while maintaining good on-eye stability.
Diagnostic fitting was not performed because the patient was non-cooperative with lens application. Thus, corneoscleral lenses were empirically ordered from keratometry and retinoscopy values. The mother was sent home with high-minus soft lenses to practice application and removal on the patient.
At the dispensing appointment, his mother was able to perform adequate application and removal technique with the corneoscleral lenses. Over-retinoscopy showed a much-improved light reflex, confirming better quality of vision with the GP optics.
Summary
In pediatric care, empirical fitting is both efficient and more tolerable to patients. With the current heightened attention being paid to infection risk and contact lenses, empirical fitting is a viable option. CLS
For references, please visit www.clspectrum.com/references and click on document #295.