



Akeratoconus (KC) patient who is successfully fit with a scleral lens (SL) may experience improved visual acuity, contrast sensitivity, and quality of life (Picot et al, 2015). Most importantly, SLs may delay the need for corneal transplantation by enabling functional vision (Ozek et al, 2018). Patients who have advanced corneal irregularity and have failed in small-diameter GP or hybrid lenses are constantly referred to our office for SLs before heading to the operating table.
After the initial fitting process, troubleshooting minor changes for an established SL wearer can be relatively straightforward. Slight distance blur? A small power adjustment will clear that up. Apical clearance getting a little too low for comfort? Let’s steepen the base curve radius a touch. We often walk out of the exam room pleased that a patient’s chief complaint has been resolved, but are we truly addressing the root cause of the symptoms?
Treat the Underlying Disease
Sometimes we can forget that these patients have a condition that, with disease advancement, may result in debilitating vision loss. So, other therapeutic interventions must be considered in addition to SL wear. Furthermore, not every patient will follow the classic presentation of KC; as many as 1 in 3 KC patients over the age of 30 experience progression (Gokul et al, 2017).
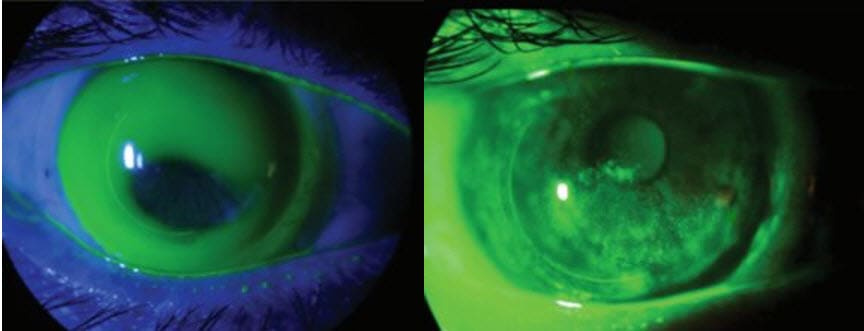
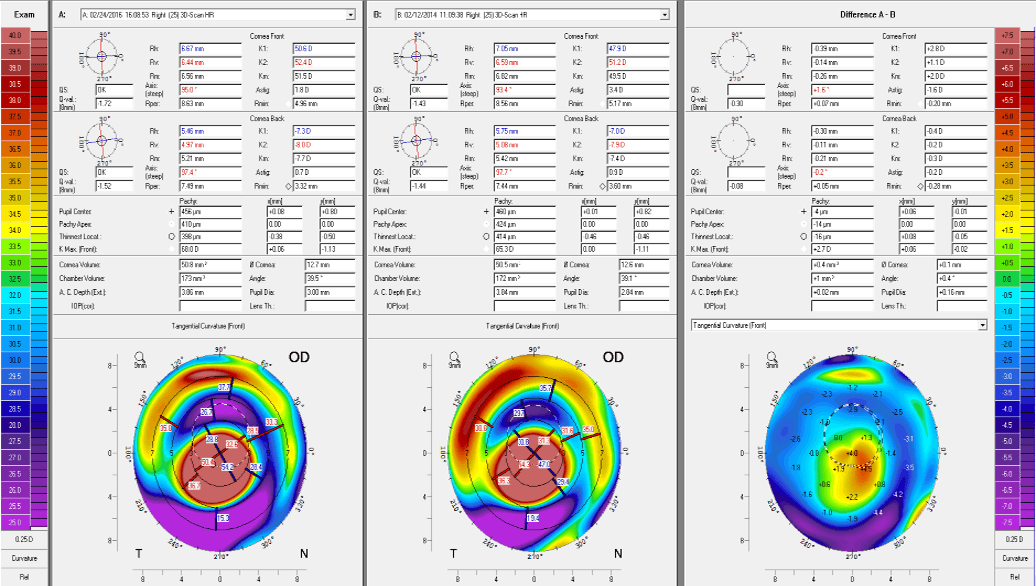
Clinical signs with SL wear that may suggest KC progression are refractive error changes despite stable internal ocular health, inadequate sagittal depth with habitual SLs (Figure 1), and progressive intolerance of SLs. You can confirm suspicions with corneal topography comparative maps (Figure 2).
I discuss corneal collagen cross-linking (CXL) with every progressive KC patient throughout the SL fitting process. The ability to “treat” KC with hard contact lenses is a common misconception, especially among patients, and it has been disproven (Barr et al, 2006). Patients need to understand that CXL is the only procedure currently available that will truly strengthen the cornea and slow or halt progressive KC and post-laser-assisted in-situ keratomileusis (LASIK) ectasia (Peyman et al, 2015). Vision preservation is largely dependent on an early diagnosis and speedy CXL referral.
At this time, there is only one U.S. Food and Drug Administration (FDA)-approved CXL procedure, and it has quickly become the new standard of care for those who have progressive KC. This quick treatment process requires epithelial debridement, a 30-minute application of two riboflavin (vitamin B2) formulations, and a 30-minute irradiance of ultraviolet-A light. Note: It is important to seek a surgeon who practices FDA-approved CXL, as it may affect patients’ long-term results and access to insurance reimbursement. Additional cross-linking drugs and devices to enable alternate treatment protocols have not been FDA-approved and are investigational.
Ideally, patients will undergo CXL prior to the SL fitting process, as postoperative corneal and scleral shape changes have been reported (DeNaeyer and Sanders, 2018; Mazzotta et al, 2012). The corneal surgeons to whom I refer do not require SL discontinuation prior to CXL. This may vary among providers.
Decreased vision, haloes, and glare are commonly experienced after surgery and should improve over time (Peyman et al, 2015; Naderan and Jahanrad, 2017). Approximately 60% of established SL wearers will require lens modifications after CXL (Visser et al, 2015). Practitioners may resume SL fitting once an epithelial defect is fully healed, and most patients may resume lens wear as early as three weeks postoperatively. The healing process can be slow; corneal curvature improvements have been noted up to four years after the initial CXL procedure in some individuals (Naderan and Jahanrad, 2017).
Summary
CXL and SLs make a powerful tool that I use frequently when faced with an ever-steepening cone. They allow me to manage my KC patients’ symptoms and provide peace of mind that there is a slowing or halting of disease progression. CLS
For references, please visit www.clspectrum.com/references and click on document #294.