



As scleral lenses (SLs) become a more widely utilized lens modality for patients who have irregular corneas or ocular surface disease, practitioners have become increasingly interested in their potential physiological impact. The International Forum for Scleral Lens Research (IFSLR), whose mission is “to advance the discipline of scleral contact lens prescribing through the coordinated efforts of evidenced-based research and clinical practice,” was held prior to the 2020 Global Specialty Lens Symposium (GSLS) in Las Vegas. This discussion-based meeting encompassed current practitioner perspectives and SL-related research. With more than 130 attendees, this meeting was a resounding success. Leading international scleral lens experts shared their extensive knowledge and debated physiological implications unique to scleral lens wear.
SESSION 1: OXYGEN
The scleral lens itself creates a barrier to direct oxygenation of the cornea from the surrounding environment, as does the fluid reservoir behind the lens. This increased oxygen barrier has the potential to compromise the cornea and may be a limitation for successful SL wear in some patients.
In this opening session, keynote speaker Clayton Radke, PhD, stated that, based on his research, if we only consider oxygen, we are oversimplifying corneal physiological events. He maintained that hypoxia—lack of oxygen—does not explain the total corneal response or, rather, the lack of response. He pointed out other metabolic events that need to be added to the equation, such as glucose metabolism and the presence of a “sink” of metabolites in the limbus.
However, the debate concerning oxygen delivery to the cornea through scleral lenses is still valid. In-vivo studies on healthy eyes versus theoretical models proved that it is not a black or white situation but more a grey area in which the individual response to hypoxic stress plays a major role.1 It is then more prudent to advocate for a measured approach when fitting scleral lenses by considering the risks and benefits for each individual patient.
The majority of clinical studies have established that corneal edema associated with SL wear varies between 1% and 3% in healthy eyes.1-3 Most study authors considered this level of hypoxia as benign and comparable with physiological overnight edema. This can be misleading, as was pointed out by Langis Michaud, OD, MSc. He noted that hypoxic stress secondary to scleral lens wear occurs rapidly, within the first 45 minutes, and persists for all wearing hours, which is not the case for physiological edema. Theoretically, the cornea can be under hypoxic stress all the time. It was also proven that all corneal layers may be impacted, mostly the stroma, but also epithelial and endothelial layers may show blebs. Karen DeLoss, OD, provided clinical data from more than 100 eyes—many with severe ocular surface disease—that indicated minimal clinically significant hypoxia in her patient cohort. She presented a few examples of complications likely related to hypoxia and emphasized the importance of long-term data from clinical populations to truly understand hypoxia during SL wear.
It was concluded that healthy eyes will probably not suffer from the low-level chronic hypoxic stress induced by SL wear in the short term. However, the story is different for eyes that have compromised tissue, especially when the endothelial cell count is low. Therefore, a balanced approach dictates that it is important to make an effort to limit hypoxic stress (lower central reservoir and lens thickness, highest material Dk) whenever possible, because we cannot always predict who will be affected.
SESSION 2: CONJUNCTIVA AND SCLERA
Knowledge of scleral shape is vital to SL fitting, and minimizing the impact of lens wear upon the conjunctival and scleral tissues is important for successful lens prescribing. The second session at the IFSLR was titled “Physiologic Considerations: Conjunctiva and Sclera.” Stephen Vincent, OD, PhD, began this session with a keynote address summarizing the numerous studies from his lab that have explored scleral topography, lens centration, and compression of the conjunctiva and sclera during SL wear.
The advent of scleral profilometry and optical coherence tomography (OCT) imaging has significantly enhanced our understanding of the interaction between the sclera and the landing zone. The Scleral Shape Study Group (SSSG) recently reported that less than 6% of scleras are spherical across a 16mm chord diameter.4 Daddi Fadel, DOptom, spoke about the importance of designing SLs that properly fit highly non-spherical scleras. She pointed out that when a spherical landing zone is applied to a toric or asymmetric sclera, lens decentration, flexure, prolapse, and fogging may result, leading to suboptimal vision or reduced comfort.5,6 A recent study by Dr. Vincent and his colleagues observed that vertical lens decentration could be minimized by reducing the thickness of the fluid reservoir, while horizontal lens decentration was primarily influenced by the horizontal scleral elevation asymmetry.7 However, a fully customized SL (e.g., bespoke corneal, limbal, and scleral zones) will ensure a uniform distribution of corneal and limbal clearance and alignment with the conjunctiva.8
Although SL designs and imaging technology have improved tremendously in recent years, there are still instances in which a fit can be challenging, especially in the presence of ocular surface irregularities such as pingueculae, pterygia, conjunctival scars, filtration blebs, and glaucoma drainage devices. Melissa Barnett, OD, discussed the management of these local obstructions and highlighted the use of impression-based technology and free-form lens designs (based on scleral mapping) to achieve a very close alignment of the scleral lens to the anterior ocular surface in the presence of significant corneal or conjunctival irregularities.
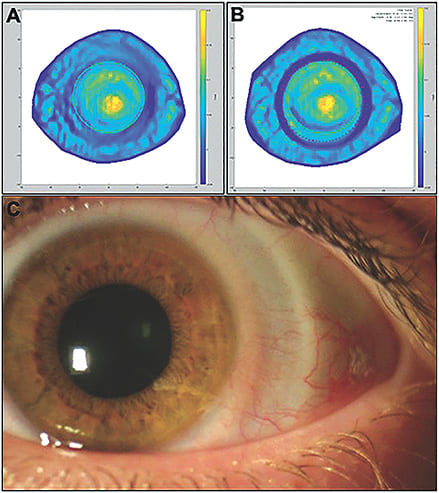
OCT imaging has also revealed that the conjunctiva bears most of the tissue compression during lens wear9 (Figure 1). The SSSG has commenced a multicenter study to determine the amount of time that it takes for complete rebound of the bulbar conjunctiva post-scleral lens removal for both neophyte and habitual lens wearers. Gregory W. DeNaeyer, OD, anticipates that this study will inform practitioners about the amount of time required for patients to cease lens wear when a refit is necessary. Tissue compression beneath the landing zone is important regarding the overall lens fit and eliminating conjunctival blanching but may also be an important consideration with respect to reported changes in intraocular pressure (IOP).
SESSION 3: INTRAOCULAR PRESSURE AND THE FLUID RESERVOIR
The final session of the IFSLR focused on the impact of SLs on IOP and the fluid reservoir beneath the lens.
Intraocular Pressure As the SL rests on the ocular tissue, it is not well understood whether the lens has any consequence with regard to the regulation of IOP. It is possible that the SL may cause compression of episcleral veins or Schlemm’s canal that may put wearers at risk of an increase in IOP and potentially at an increased risk for glaucoma. As early as the 1950s, Ascher observed that glass SLs altered aqueous outflow from Schlemm’s canal to the episcleral venous network.7 More recently, several experts have suggested that modern scleral lenses may cause IOP to elevate, and others have tested the hypothesis using various techniques.10-15
The session began with a keynote from Cherie Nau, OD, who discussed the current literature assessing the effect of SLs on IOP. She noted that these studies have used various measurement techniques, lens designs, sample sizes, and wearing protocols and, thus, have yielded inconsistent results. For example, two studies measured IOP with the lens on the eye; both used the Diaton (DevelopAll Inc.) transpalpebral tonometer, and both reported an average increase in IOP after four to eight hours of lens wear.14,16 In contrast, Dr. Nau discussed her own study, which used a pneumatonometer to measure IOP during SL wear in 29 subjects. She noted little change in IOP after two hours of lens wear.13 Dr. Vincent and his group used two different measurement techniques (non-contact tonometry [NCT] and ocular response analyzer) and had different sample sizes and SL wear duration, but they found a decrease in IOP when using the same type of lens in two normal cohorts.11 Another study by Aitsebaomo et al measured an increase in IOP after eight hours of lens wear in nine young non-SL wearers when measuring IOP with an Icare (Icare USA) tonometer;12 however, their data shows a few subjects who had quite high IOP that could have skewed the average increase. Table 1 summarizes all current studies assessing IOP during SL wear.
| MEASUREMENT | AUTHOR(S)/YEAR | AGE | HABITUAL SL WEAR | LENS ON OR OFF FOR IOP | N (EYES) | SIZE OF LENS (MM) | HOURS OF LENS WEAR | CHANGE IN IOP (mmHg) |
|---|---|---|---|---|---|---|---|---|
| Ocular Response Analyzer (ORA)* | Vincent et al, 2017 |
21 to 33 | No | Off | 7 | 16.5 | 3 | –1.3 |
| Non-Contact Tonometer | 18 to 32 | No | Off | 5 | 16.5 | 8 | –0.4 | |
| Icare** | Aitsebaomo et al, 2019 | 18 to 35 | No | Off | 9 | 15.8 | 8 | 5.8 |
| Tonopen* | Shahnazi et al, 2019 | 57 ± 17 | Yes (OSD) | Off | 46 | 17.0 and 18.0 | 1 to 8+ | –0.89 |
| Diaton*** | Turpin et al, 2018 | Unknown | No | On | 14 | 14.6 to 15.2 | 8 | 5.5 |
| Diaton | Michaud et al, 2019 | 25 ± 4 | No | On | 21 | 15.0 18.0 |
4.5 4.5 |
4.4 5.2 |
| Pnuematonometer* | Nau et al, 2016 | 29 ± 6 | No | On | 29 | 15.0 | 2 | 0.3 |
| * Reichert ** Icare USA *** DevelopAll Inc | ||||||||
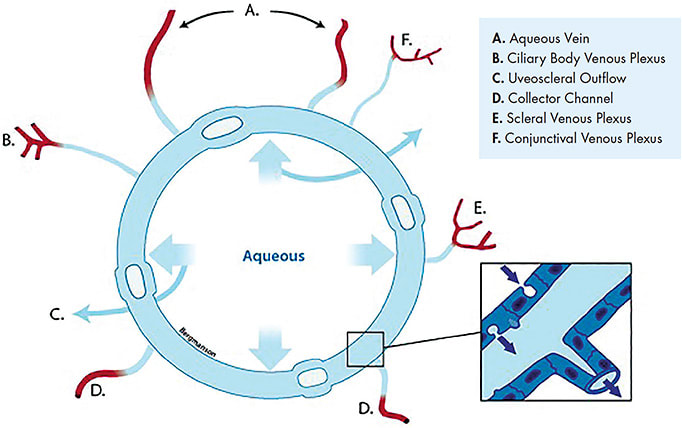
According to Pearson, the idea that SLs potentially elevate IOP is as old as the lens itself.17 However, it was pointed out that aqueous has four different routes to escape from the eye, and it should be considered that the outflow system may have enough flexibility to accommodate an impediment of drainage through external route(s) (Figure 2). The validity of IOP measurements from the sclera using instruments calibrated on the cornea was discussed by Jan Bergmanson, OD, PhD, who provided a thorough review of the structural differences between the cornea and sclera. So far, there appears to be no definitive answer on how SLs may affect IOP. This is an area of research that needs to continue to be investigated, preferably with some agreement on preferred instrumentation and protocol. Until we better understand how SLs may influence IOP, patients should be checked for glaucoma.
Tear Fluid Reservoir The fluid reservoir (FR) beneath an SL provides a great benefit to patients who have a debilitating eye disease. One SL indication is for use as a treatment for severe dry eye to improve signs and symptoms. However, Gonzalo Carracedo, PhD, reminded us that in his research involving keratoconus patients, tear film parameters—such as volume, stability, and pro-inflammatory molecule concentrations—worsen with SL wear. Moreover, the ocular surface shows reduced wettability after SL wear, which suggests that artificial tear drops could be recommended after SL removal.
However, dry eye symptoms and comfort perception improved in this population after SL wear. Dr. Carracedo suggested that the disconnect between objective and subjective perception could be due to the dramatic visual acuity improvement with SLs, which is known to be a key factor in biasing patient evaluation of comfort.
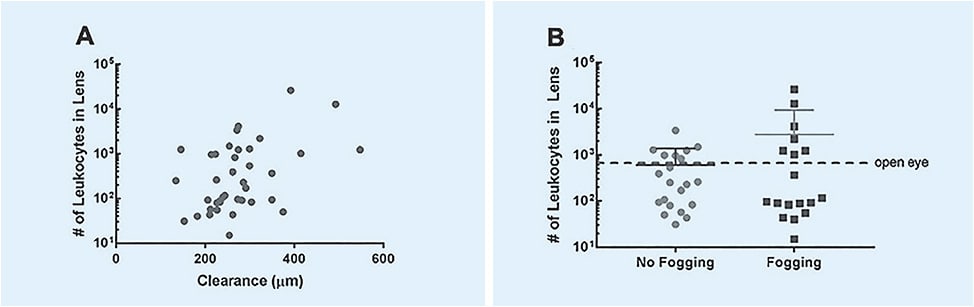
The composition of the FR was also discussed, mostly in the context of midday fogging (MDF). MDF occurs in approximately 30% of patients when debris accumulates in the FR during lens wear.18,19 MDF limits visual acuity, necessitates more frequent SL removal and handling, and has been reported as the most common scleral lens complication in most practices. Jason Nichols, OD, MPH, PhD, presented data showing an increase in leukocytes in the FR during MDF (Figure 3), an observation that suggests that MDF has inflammatory properties. The audience was also reminded that leukocytes exponentially increase overnight when the eye is closed, and a comparison of the scleral lens FR to the closed eye tear environment was offered. This study and others have confirmed that a thicker FR layer is a risk factor for developing MDF.20 Another risk factor may be tight lenses, although conjunctival compression has not been correlated to MDF in any clinical trials.17
The discussion continued as Maria Walker, OD, MS, presented data showing that total protein and lipid content were increased in MDF, although several matrix metalloproteinases (MMP-2, -3, -7, -9, and -10) were not.
Overall, these presentations suggested that there is an increased inflammatory presence in MDF, with a greater presence of inflammatory cells in the FR; however, no specific inflammatory proteins or lipids have been identified, and the physiological consequences of this phenomenon remain poorly understood.
CONCLUSION
The assembly of experts at the IFSLR, both as presenters and attendees, allowed for a dynamic discussion of several research topics related to SLs. A robust understanding of these topics is important to evolve the SL field. We look forward to the next meeting of the IFSLR on Jan. 20, 2021 prior to the start of the 2021 GSLS. CLS
Acknowledgement: The authors would like to acknowledge all of the IFSLR presenters who have provided the content for this article as well as the Global Specialty Lens Symposium and Contact Lens Spectrum for partnering with the IFSLR to make this program possible.
REFERENCES
- Compañ V, Oliveira C, Aguilella-Arzo M, Mollá S, Peixoto-de-Matos SC, Gonzalez-Meijome JM. Oxygen diffusion and edema with modern scleral rigid gas permeable contact lenses. Invest Ophthalmol Vis Sci. 2014 Sep;55:6421-6429.
- Tan B, Tse V, Kim YH, Lin K, Zhou Y, Lin MC. Effects of scleral-lens oxygen transmissibility on corneal thickness: A pilot study. Contact Lens Anterior Eye. 2019 Aug;42:366-372.
- Vincent SJ, Alonso-Caneiro D, Collins MJ, et al. Hypoxic Corneal Changes following Eight Hours of Scleral Contact Lens Wear. Optom Vis Sci. 2016 Mar;93:293-299.
- DeNaeyer G, Sanders DR, van der Worp E, Jedlicka J, Michaud L, Morrison S. Qualitative Assessment of Scleral Shape Patterns Using a New Wide Field Ocular Surface Elevation Topographer: the SSSG Study. JCLRS. 2017 Nov 16;1:12-22.
- Vincent SJ, Fadel D. Optical considerations for scleral contact lenses: A review. Cont Lens Anterior Eye. 2019 Dec;42:598-613.
- Fadel D. Scleral Lens Issues and Complications Related to a Non-optimal Fitting Relationship Between the Lens and Ocular Surface. Eye Contact Lens. 2019 May;45:152-163.
- Kowalski LP, Collins MJ, Vincent SJ. Scleral lens centration: The influence of centre thickness, scleral topography, and apical clearance. Cont Lens Anterior Eye. 2019 Dec 10;S1367-0484(19)30325-X. [Online ahead of print]
- Ascher KW. Aqueous veins and contact lenses. Am J Ophthalmol. 1952 May;35:10-20.
- Alonso-Caneiro D, Vincent SJ, Collins MJ. Morphological Changes in the Conjunctiva, Episclera and Sclera following Short-term Miniscleral Contact Lens Wear in Rigid Lens Neophytes. Cont Lens Anterior Eye. 2016 Feb;39:53-61.
- McMonnies CW. A Hypothesis that Scleral Contact Lenses could Elevate Intraocular Pressure. Clin Exp Optom. 2016 Nov;99:594-596.
- Vincent SJ, Alonso-Caneiro D, Collins MJ. Evidence on Scleral Contact Lenses and Intraocular Pressure. Clin Exp Optom. 2017 Jan;100:87-88.
- Aitsebaomo A, Wong-Powell J, Miller WL, Amir F. Influence of Scleral Lens on Intraocular Pressure. JCLRS. 2019 Apr 22;3:e1-e9.
- Nau CB, Schornack MM, McLaren JW, Sit AJ. Intraocular Pressure after 2 hours of Small-Diameter Scleral Lens Wear. Eye Contact Lens. 2016 Nov;42350-42353.
- Michaud L, Samaha D, Giasson CJ. Intra-ocular Pressure Variation Associated with the Wear of Scleral Lenses of Different Diameters. Cont Lens Anterior Eye. 2019 Feb;42:104-110.
- Shahnazi KC, Isozaki VL, Chiu GB. Effect of Scleral Lens Wear on Central Corneal Thickness and Intraocular Pressure in Patients With Ocular Surface Disease. Eye Contact Lens. 2019 Oct 24. [Online ahead of print]
- Turpin S, Antoniuk K, Caroline P, et al. Does IOP Increase During Scleral Lens Wear? Poster presented at the Global Specialty Lens Symposium, January 2018, Las Vegas.
- Pearson RM. Re: A hypothesis that scleral contact lenses could elevate intraocular pressure. Clin Exp Optom. 2017 Jan;100:103-104.
- McKinney A, Miller W, Leach N, Polizzi C, van der Worp E, Bergmanson J. The Cause of Midday Visual Fogging in Scleral Gas Permeable Lens Wearers. Invest Ophthalmol Vis Sci. 2013 Jun;54:5483.
- Walker M, Bergmanson JP, Marsack JD, Miller W, Johnson L. Complications and fitting challenges associated with scleral contact lenses: A review. Cont Lens Anterior Eye. 2016 Apr;39:88-96.
- Postnikoff CK, Pucker AD, Laurent J, Huisingh C, McGwin G, Nichols JJ. Identification of leukocytes associated with midday fogging in the post-lens tear film of scleral contact lens wearers. Invest Ophthalmol Vis Sci. 2019 Jan;60:226-233.