


Post-Penetrating Keratoplasty GP Fitting
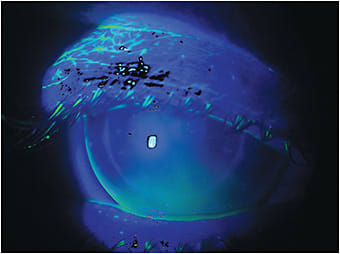
Figure 1 shows a case of post-penetrating keratoplasty (PK) in which the patient was fit with an aspheric, intralimbal GP lens with an overall diameter of 12.5mm on his right eye (OD).
Although the lens of choice in a highly complex case such as this may be a scleral lens, a number of such patients in our practice prefer corneal GP lenses; most have already been wearing corneal GPs for a long time after their surgery. The difficulty with post-PK cases is that the result is always unpredictable and is dependent on surgeon skills or surgery planning and also on the placement of the sutures and on the individual graft cicatrization of each cornea. In most cases, we find highly asymmetrical, irregular astigmatism associated with an elevation of the central cornea in a plateau followed by a more curved corneal periphery.
Scleral lenses work well in these cases. Some practitioners are wary to fit a scleral lens over a corneal transplant, but if the scleral lens is well designed—not too thick, with a ventilation channel—and specular microscopy shows a cell density of more than 700 cells/mm2, it is a safe fit. Customized scleral lens design results in better overall alignment with the cornea and a smooth landing over the scleral conjunctiva.
Things get more complex when it is necessary to fit post-graft patients with corneal GPs. It is necessary to plan and customize a corneal GP design to provide comfort, the best possible centration and stabilization during blinking, and especially to maintain the cornea’s physiological balance with the best possible visual acuity.
History
This 47-year-old male first came to our clinic in 2000. He had a history of keratoconus and recurrent corneal erosion due to corneal touch at the apex with lens wear. He was refit during the following years with lenses that had steeper base curves to avoid apical touch, with the exception of 2007, at which time he left our clinic to obtain lenses elsewhere that caused apical touch but that he thought provided better visual acuity. He returned to our care after developing a corneal ulcer with the flatter lenses.
His most recent refit at our clinic was in 2010. After that, we didn’t see him again until June 2020. He had undergone PK OD in 2016. The doctor who performed the surgery tried to fit him with a scleral lens and also with a corneal GP lens, but the patient could not tolerate the lens on the eye. He made it clear that he wanted to be fit with a corneal GP, if possible, and not with a scleral lens.
On his left eye, he was still wearing the lens that was fit in 2010. There was mild apical touch, so we adjusted the specialty keratoconus design specifications to better align the lens over the cornea and to avoid apical touch. The lens had a 69.50D x 48.00D double base curve, with an 11.4mm overall diameter.
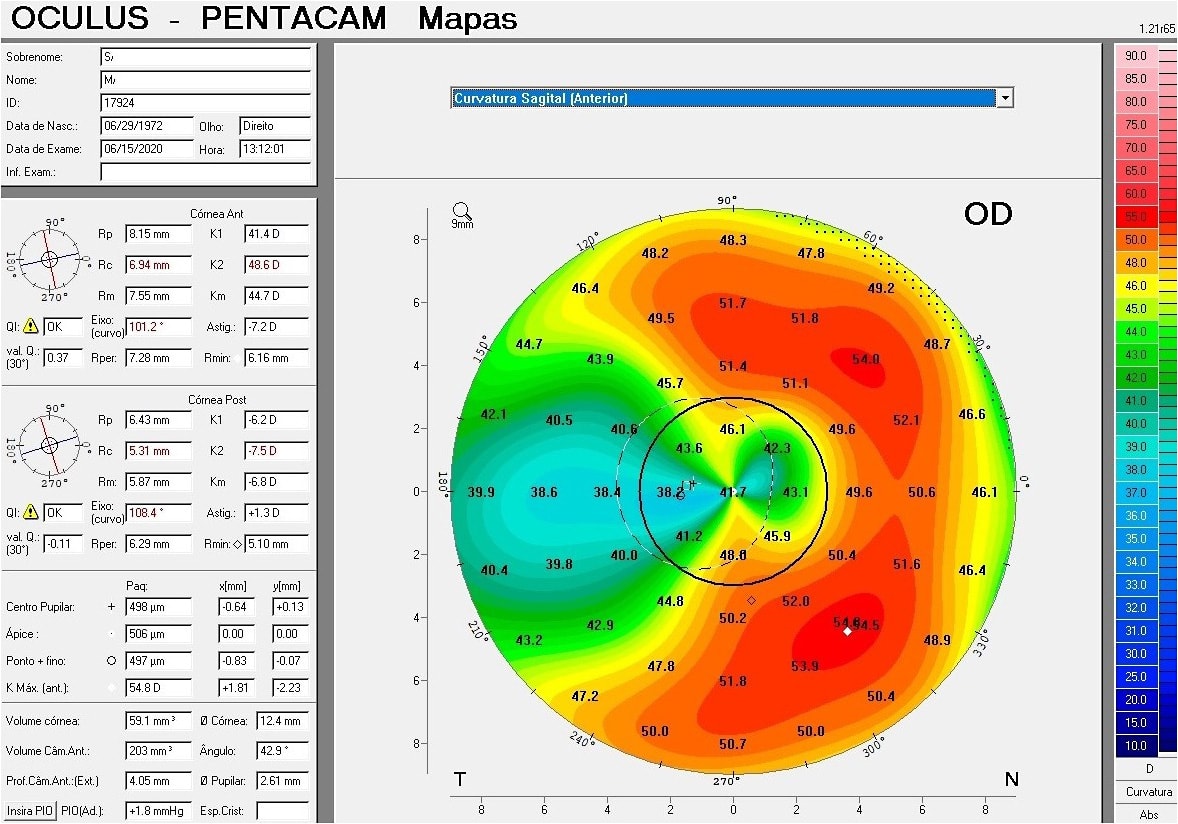
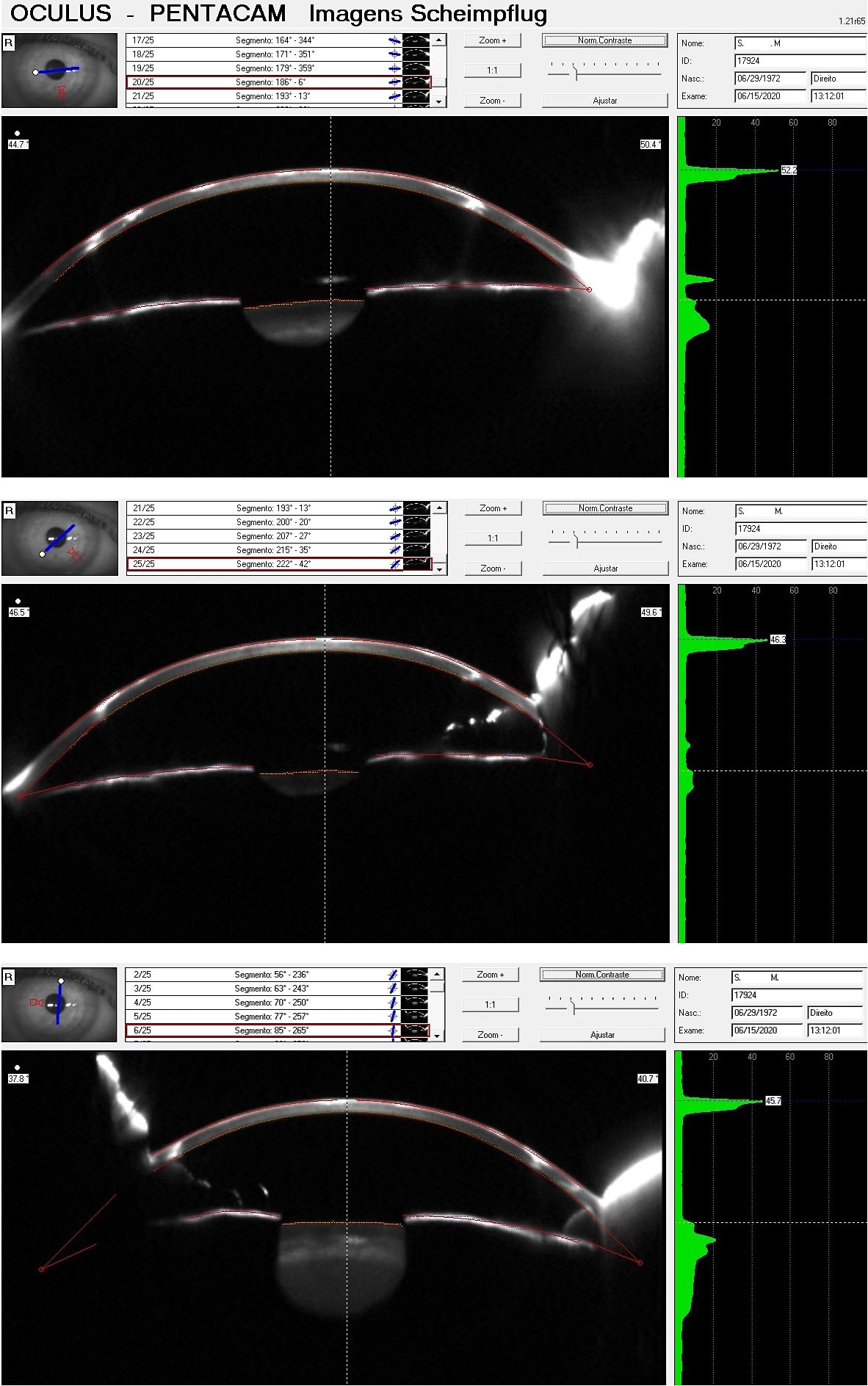
The PK OD resulted in high irregular astigmatism (Figure 2), but it was still possible to try a corneal GP lens. Figures 3 through 5 show the differences at the vertical, oblique, and horizontal angles.
Corneal Biomicroscopy
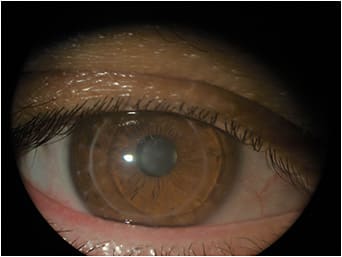
Initial slit lamp observation showed a well-sutured graft, with a few remaining stiches at 6 o’clock. The overall aspect was good, with no corneal opacities or neovascularization (Figure 6). The anterior corneal curvature was not as irregular as in similar cases, but the presence of the graft and the trephination1 incision makes the central and paracentral cornea more complex and challenging for corneal GP lens fitting. To avoid touch at the apex and to provide clearance over the graft, it is important to estimate the graft size,2 as these vary in diameter.
To calculate the initial trial lens, we took the medium K (Km) and added 1.00D steeper; the result was a large, intralimbal aspheric lens with parameters of 46.00D base curve (BC), 12.0mm overall diameter (OAD), and –8.00D power (Figure 7). The trial lens resulted in some air bubbles that would reach the lens center, which will compromise vision and possibly cause some discomfort during wear. At the horizontal meridian, we increased the aspherical eccentricity to prevent 3 o’clock and 9 o’clock staining at the peripheral cornea.
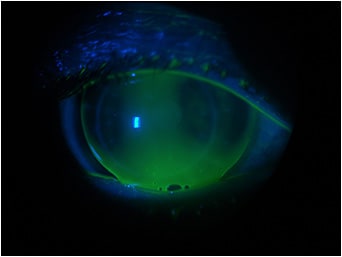
The final ordered lens had parameters of 46.50D BC, 12.5mm OAD, –8.75D power, Optimum Extra (Contamac) material (Dk 100). This lens exhibited central clearance, good centration, better alignment, and stability (Figure 1). Figure 8 shows the slit lamp observation with the cross-section view with a nice alignment at 90°. The patient was comfortable with the lens, and although there are areas of intermediate and peripheral fluorescein pooling at 90° and a more visible flatter area along the horizontal meridian, the lens presented an adequate fluorescein pattern indicating that it would prevent any risk to the graft or insult to the graft edge.

I designed a lens with a higher, wider peripheral eccentricity and an edge lift flat enough to allow lacrimal exchange. It is important to note that the lacrimal pump in an intralimbal design is not the same as in standard corneal lenses. For this reason, it is also important to use a high-Dk material; but again, it depends more on the design than on the permeability of the material.
There are some other factors to consider when fitting a post-PK cornea. Fitters must understand how wide the peripheral curve should be and how much edge lift there should be—not necessarily in actual numbers, but it is important to understand what modifications are required to achieve a successful result. In this process, the help of a specialty lens consultant at a reliable laboratory is of great importance. Digital imaging and video recordings of trial lenses can help both practitioners and lab consultants.
Conclusion
Corneal GP lens fitting is here to stay. No matter how remarkable scleral lenses are, there will be always patients and cases for which the best option will be corneal GPs. It is not necessary to have a lot of trial lens sets from different contact lens manufacturers to succeed with these fittings; in our experience, too much variety can confuse the process. It is ideal to have two reliable labs that you can trust to offer high-quality corneal GPs and also the resources to implement design modifications when necessary.
Know that fitting specialty GP lenses involves a learning curve and an experience curve. You can’t succeed if you don’t try. If you fail, go back to the beginning and apply the modifications that you believe will succeed. In these cases, it is also important to communicate effectively with patients to make sure that they understand that they may need to come to your office more often due to the complexity of their case. If you manage patients well, they will be willing to collaborate with you.
References
- Seitz B, Langenbucher A, Naumann GOH. Trephination in Penetrating Keratoplasty. In Essentials in Ophthalmology: Cornea and External Eye Disease, Reinhard T, Larkin DFP, eds. Springer-Verlag Berlin Heidelberg, 2006. Available at http://eknygos.lsmuni.lt/springer/104/123-152.pdf . Accessed Sept. 1, 2020.
- Goble RR, Hardman Lea SJ, Falcon MG. The use of the same size host and donor trephine in penetrating keratoplasty for keratoconus. Eye(Lond). 1994;8(Pt 3):311-314.
