



Are you reading this article on your computer, your phone, or in the print issue that you just received in the mail? Is there one mode that you prefer over the others? Regardless of its form, you can still enjoy the content. The same can be said for the process of prescribing orthokeratology (ortho-k). There are different fitting methods to achieve ideal results. Each one can result in a great outcome, but you have to be comfortable with the level of technology that best fits you.
Diagnostic For those who enjoy seeing and “getting the feel of” the fit, you may prefer to prescribe based on your evaluation during a diagnostic assessment of a known lens. With this method, initial fitting depends on your skill in reading the fluorescein pattern. Also, while observing the lens on the eye, you can assess a patient’s reaction to wearing the lens.
Empirical Another option is to order the initial ortho-k lens empirically; no diagnostic evaluation is required. A practitioner sends the pertinent exam data to the lab: the K readings (or simulated keratometry from topography), refraction, and corneal diameter; some may also ask for eccentricity. This is a more “hands-off” approach that removes the decision-making about the initial lens design from the practitioner. Manufacturers using this system have accumulated data from numerous patients to produce successful designs from the provided findings.
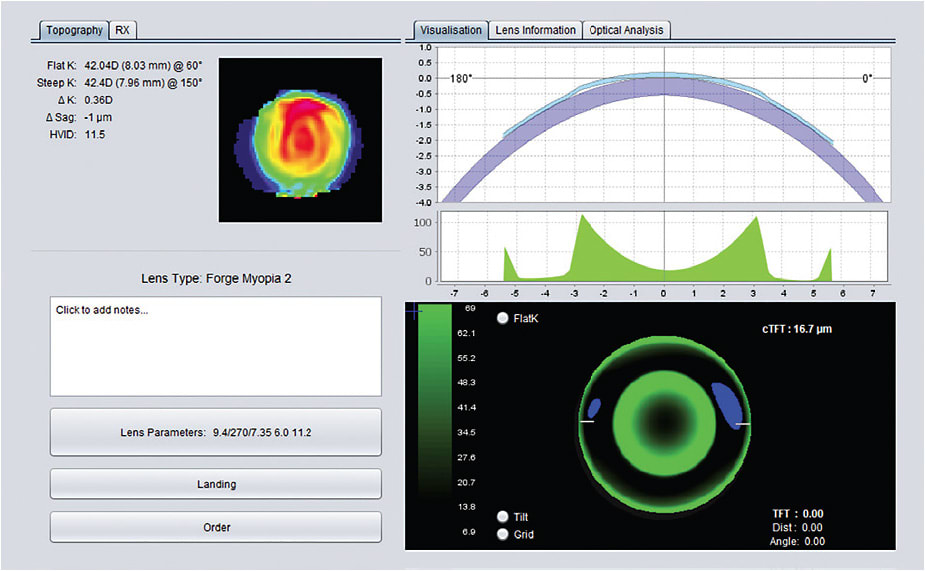
Design Software Some practitioners may want a more tech-oriented perspective. This method imports a patient’s baseline topography into a design software program. Once the refraction is entered, the system will generate a lens design or produce an image of a “virtual” diagnostic fitting by simulating a fluorescein pattern with a specified lens design (Figure 1). The practitioner may then order the software-generated design or specify a customized design based on prescribing preferences for that patient. Because the fitting is based on corneal mapping, a high-quality baseline topography is essential.
Getting an Ideal Fit
But, what happens if the initial lens does not produce ideal results? Just as initial lens ordering is different with each of the above methods, so is the process of problem-solving. With the diagnostic method, re-evaluation of additional diagnostic lenses will be needed. In the empirical system, contacting a manufacturer’s consultant is necessary to determine which parameter changes will solve the issue. And with the design software, revisiting the initial analysis (both topography and design) is required. The common thread with each of these techniques is found in corneal topography. In ortho-k, the technology and data provided by corneal topography are essential to establishing a baseline starting point and to monitoring treatment.
As we consider how to provide eyecare services with a minimum of patient visits, remember that ortho-k is a specialized process and a service that requires patients to be seen in the office for careful instruction in lens handling, follow-up topography, and careful slit lamp evaluation. The next breakthrough for ortho-k may involve applying smartphone technology for patients to capture high-quality anterior segment images as well as topography of their own eyes, which are then sent to you. For now, keep using the technology of corneal topography for safety and success in ortho-k. CLS