



Specialty contact lenses are incredibly rewarding, enabling practitioners to help patients achieve excellent vision and comfort. However, learning the nuances of how to properly bill and code for these lenses can be tedious, time consuming, and frustrating. When I entered private practice immediately following my residency, I joined a clinic that had no experience at all with specialty lenses. It was my job to help the staff, and together, with some trial and error, we developed a system. Here, I will outline my recommended steps for a successful fitting process and proper coding and billing.
CONSULTATION
Any clinic wanting to get involved with specialty contact lenses should set up a schedule for new patient consultations. These would be for any new patients interested in specialty contact lenses or for patients referred to you for a medically necessary contact lens.
When I first started practicing, I would schedule about one-to-two hours for these consultations. I assumed that patients would come in for a consultation and then proceed with a contact lens fitting. One or two hours appeared to be sufficient time to perform the consult, work-up evaluation, and fitting. There were many problems with this system. First—no shows! Any patient who did not show up would mean a large gap in the schedule. This is inefficient and counterproductive to the clinic and to staff flow.
The next problem was that some patients who came for the consultation did not want to proceed with a contact lens fitting. Some patients were good candidates for medically necessary contact lenses, but the cost was too high. Others were good candidates, but the thought of wearing a contact lens was unappealing to them (not sure why such patients come for a contact lens consult). So, a large amount of work would go into the consultation and work-up for such patients, and then they would not even get contact lenses. What a waste of time!
Another issue that arose with this system was that the staff would determine the insurance benefits based on a diagnosis that a patient or another practitioner provided, but then examination would reveal that the patient had a completely different diagnosis, and the insurance process would need to be repeated all over again. For instance, let’s say that a patient gets referred to you for keratoconus. Your staff does all of the work to determine whether that diagnosis is covered by the patient’s insurance plan with that code, etc. Then you find that the patient actually has radial keratotomy scarring, not keratoconus. You now have to verify coverage with the insurance company for the new diagnosis.
The last issue that we experienced involved patients who were referred for a medically necessary contact lens consult, but they did not need that type of fitting at all. For example, a patient was once referred for a contact lens consultation because of suspected keratoconus. However, an analysis of the data indicated that the patient actually had glaucoma. So, another wasted hour for everyone involved.
After several of these experiences, we changed our consultation time to 15 minutes. A staff member takes a case history; performs topography, pachymetry, and fundus photography; and checks vision. Then, I perform a slit lamp examination, review my findings with patients (Figure 1), and discuss their options.

When patients want to proceed with specialty lenses, I schedule them to return for a one-hour fitting. This flow has proven to be much more efficient for everyone involved at our practice.
ONCE THE CONSULTATION IS COMPLETE
Once you have performed the consultation, you now have the proper diagnosis codes for the staff to contact the insurance companies to obtain prior authorization. The consult is also a great way to determine what contact lens would work best for a patient. Once you’ve seen a patient, discussed all of the options, and scheduled him or her for a fitting, you can now determine—via the insurance carrier—what is covered. By scheduling patients to return one-to-two weeks after the consult, your staff has enough time to collect the insurance information and to notify you or the patient as to whether there are any issues before the next appointment.
Items needed to determine insurance eligibility for a patient are:
- Name of patient’s vision and medical insurance plans
- Patient’s name, date of birth, and insurance ID number(s)
- Diagnosis and associated International Classification of Diseases (ICD) code(s)
- Fitting Common Procedural Terminology (CPT) codes
- Material V codes
- Usual, customary, and reasonable (UCR) service fees
You’ll want to check both a patient’s vision and medical insurances, as there may be one insurance that covers the ICD and the CPT codes while the other does not. For example, perhaps a scleral lens fitting is not covered by a patient’s medical plan, but it is covered by his or her vision plan.
Once you have all of the previously mentioned items, you are ready to verify a patient’s insurance benefits. Some insurances can be verified easily online; others you will have to call.
When calling an insurance company, here is a sample of what staff members should include in the conversation: “Hi, I am calling from Dr. Stephanie Woo’s office, provider number 1234567. We are calling to verify coverage on a service and material. The patient’s name is ______, and his/her member ID is ______. Can you please let me know whether CPT code 92072 (keratoconus contact lens fitting) is a covered service? The diagnosis code would be H18.613 (keratoconus, stable, bilateral). If it is covered, what is the expected reimbursement?”
It is important to let the insurance company know the CPT code that you intend to use (i.e., which type of contact lens fit you want to perform) and also any relevant ICD 10 codes. It is always best to give them as many codes as possible. For example, a scleral lens may not be a covered service for corneal scarring (H17.813), but it might be a covered service for punctate keratitis (H16.143). For this reason, have any relevant ICD 10 codes available. You may be surprised at what is covered.
I also recommend asking the insurance provider what the expected reimbursement is. Sometimes the reimbursement is less than what the cost of the material is to you! In this case, you would be losing money if you relied only on insurance reimbursement. These are all important pieces of information to collect prior to proceeding with any contact lens fitting.
RELEVANT CPT CODES
CPT codes are used to bill a patient’s medically necessary contact lens fitting. You or your office sets your UCR fees.
The following are common CPT codes used for contact lens fittings:1
92310 (Prescription of Optical and Physical Characteristics of and Fitting of Contact Lens, with Medical Supervision of Adaptation; Corneal Lens, Both Eyes, Except for Aphakia): Use this code when fitting any corneal lenses, including standard soft contact lenses, custom soft lenses, soft toric lenses, soft multifocal lenses, corneal GP lenses, intralimbal lenses, and hybrid lenses.
92311 (Prescription of Optical and Physical Characteristics of and Fitting of Contact Lens, With Medical Supervision of Adaptation; Corneal Lens for Aphakia, One Eye): This code is for the fitting of any corneal lens for unilateral aphakia.
92312 (Prescription of Optical and Physical Characteristics of and Fitting of Contact Lens, With Medical Supervision of Adaptation; Corneal Lens for Aphakia, Both Eyes): Use this code when fitting any corneal lens for bilateral aphakia.
92313 (Prescription of Optical and Physical Characteristics of and Fitting of Contact Lens, With Medical Supervision of Adaptation; Corneoscleral Lens): This code applies to fitting of a corneoscleral or a scleral lens (currently there is no code available specifically for full scleral lenses).
92072 (Fitting of Contact Lens for Management of Keratoconus, Initial Fitting): Use this code when fitting any lens for a patient who has keratoconus (must verify specific keratoconus classification guidelines with insurance provider). Refer to the provider manual for subsequent fittings (some insurances will pay this code only once for the lifetime of the patient, and subsequent fittings will require a different fitting code such as 92310). Most insurance companies will allow you to bill this code every year when you see a keratoconus patient.
92071 (Fitting of Contact Lens for Treatment of Ocular Surface Disease): This code applies to fitting a contact lens to manage ocular surface disease. Right/Left eye can be specified with the appropriate modifier (i.e., 92071-RT). I tend to reserve this code for when I use a bandage contact lens to treat diseases such as superficial punctate keratitis, corneal abrasions, recurrent corneal erosions, dry eye, etc. Note: You should not report both 92071 and 92072 codes together.2
With some insurance companies, there may be only a set of CPT codes from which to select. It is best to consult with the company to determine the most appropriate code for your specific case. Be sure to obtain the reference code and name of the representative with whom you spoke if you are collecting information over the phone.
SOME CODING CONUNDRUMS
Because 92310 is the only code appropriate for most soft contact lens fittings and for some GP lens fittings, how do you designate different pricing for different tiers of service? Usually, each CPT code is assigned one fee. This is where it can become complicated, because different lens fittings in this category require different levels of service. In my office, we use the following internal modifiers:
- 92310-1: soft contact lens fitting, sphere
- 92310-2: soft contact lens fitting, toric
- 92310-3: soft contact lens fitting, multifocal
- 92310-4: corneal GP fitting, sphere
- 92310-5: corneal GP fitting, bitoric
- 92310-6: corneal GP fitting, multifocal
- 92310-7: hybrid lens fitting, sphere
- 92310-8: hybrid lens fitting, multifocal
Each modifier corresponds to a different fee, and that will display at the checkout area when patients pay their bill for the day.
What if none of the CPT codes match the type of lens that I am fitting? When none of the CPT codes seem appropriate, you can call the insurance company to guide you. Be sure to get the representative’s name and reference number. If none of the CPT codes seem appropriate, you can bill a miscellaneous code, but most insurances will not reimburse these codes (or they reimburse very little).
V codes V codes are used to bill the contact lens material. In most cases for which the material supply is billed separately, each unique contact lens type has a specific V code to bill.
Common V codes used for medically necessary contact lenses include:1
V2510—Contact Lens, GP, Spherical, Per Lens
V2511—Contact Lens, GP, Toric, Per Lens
V2512—Contact Lens, GP, Bifocal, Per Lens
V2513—Contact Lens, GP, Extended Wear, Per Lens
V2520—Contact Lens, Hydrophilic, Spherical, Per Lens
V2521—Contact Lens, Hydrophilic, Toric, Per Lens
V2522—Contact Lens, Hydrophilic, Bifocal, Per Lens
V2523—Contact Lens, Hydrophilic, Extended Wear, Per Lens
V2531—Contact Lens, GP, Scleral, Per Lens
V2599—Contact Lens, Other Type (hybrid)
V2627—Scleral Cover Shell
V2799—Miscellaneous Vision Item or Service
Modifiers can be used to designate the quantity as well as the right and left eye. For example, V2599-RT quantity 2 (assuming that the insurance plan allows for an annual supply) would mean that you are billing an annual supply (six-month replacement) of hybrid lenses for the right eye.
A BILLING EXAMPLE
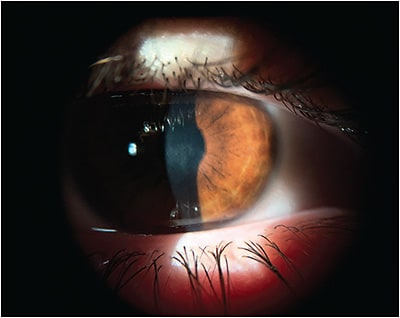
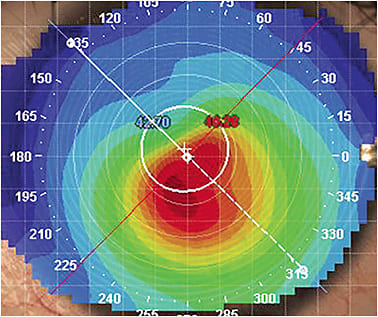
A 45-year-old female presented to the clinic for a consultation for keratoconus. Best-corrected spectacle acuity was 20/60 with the right eye and 20/70 with the left eye. Her slit lamp examination showed inferior-central thinning in both eyes along with striae and scarring in both eyes (Figure 2A). Figure 2B shows her topography. We reviewed the pros and cons of different lens modalities, and she opted for a scleral lens fitting in both eyes to improve her visual quality. She had medical and vision insurance. We scheduled her for a one-hour scleral lens fitting about one week later.
Now that I had evaluated the patient, I was ready to give the proper codes to the staff so that they could start researching her insurance benefits. Here are the codes that I gave them:
- CPT code 92072 (keratoconus contact lens fitting) or 92313 (corneoscleral lens fitting)
- V2531-RT and V2531-LT (scleral lens right eye and left eye, respectively)
- ICD 10 codes: H18.613 (keratoconus, stable, bilateral), H17.113 (central corneal scar, bilateral)
- UCR fees for the CPT codes and the V codes
A staff member called the vision plan and the medical plan. She found that both insurances covered the CPT code 92072, but only the vision plan would cover 92313. The V codes were covered by the vision plan but not by the medical plan. In this case, because the vision plan was able to cover both the fitting and the contact lens material, we opted to bill the patient’s vision insurance. The patient returned to the clinic for her scleral lens fitting, and then we billed her vision insurance.
Note: A VSP billing specialist with whom I spoke indicated that the contact lens fitting should not be billed until the fitting process, follow-up care, lens changes, etc., are complete. This can be the case with many vision plans. If you are unsure when to bill a fitting, it is best to consult with an insurance representative from the specific plan.
HOW DO I KNOW WHAT TO CHARGE?
This is a common question. While I cannot make specific recommendations, there are a few tools and resources that can help practitioners establish fees in their own clinic.
The GP Lens Institute (GPLI) has a free calculator on its website at www.gpli.info/professional-fee-calculator . Simply plug in the information, and the calculator suggests pricing for you.
I developed a tool to help practitioners determine their own fees as well. This calculator, available at www.drstephaniewoo.com/calculate-my-fees , is also free and is simple to use.
Practitioners can also do the math themselves if they know their chair time cost. As an example with an easy, round number, let’s say that your chair time is $100 per hour. You would multiply this by the number of hours that you expect to spend with a given patient. If you anticipate spending four hours with a specialty lens patient (one hour for the fitting, one hour for the dispense, and four follow-up visits at 30 minutes each), then you would multiply your chair time cost of $100 by 4, which would be $400 for that patient. Make sure that you charge at least that amount, because if you choose to not fit the specialty lens patient, you would use that time to perform regular eye examinations that would generate the same amount of income.
ADDITIONAL RESOURCES
There are many different resources aimed at helping practitioners with billing and coding for specialty lenses.
Organizations The Scleral Lens Education Society (SLS) and the GPLI are both nonprofit organizations that provide resources to practitioners and staff. Both organizations offer webinars, many of which involve the topic of billing and coding. These webinars are free and are often archived, so you can view them at a later date. The GPLI has a module devoted to coding and billing of specialty lenses at www.gpli.info/coding-billing .
Publications Many professional publications feature helpful articles written by experts in the industry, some of which cover coding and billing of specialty lenses and other business aspects of contact lens practice.
Live Education Many eyecare conferences hosted by eyecare organizations as well as contact lens-specific conferences such as the Global Specialty Lens Symposium offer courses specifically pertaining to or emphasizing billing and coding.
Webinars Many eyecare education companies offer webinars or virtual continuing education events.
Billing Services There are a variety of billing services aimed to help answer practitioners’ questions about coding and billing and to provide billing assistance.
Contact Lens Manufacturers This is a hugely under-used service! If you are having problems with billing and coding of a medically necessary contact lens, reach out to the contact lens manufacturer. Some manufacturers have an employee on staff who can directly assist with billing, or manufacturers can direct you to an expert within the field. Many have written resources or webinars on this exact topic. Keep in mind that manufacturers want to help you! They don’t succeed if you don’t succeed. They will do everything in their capacity to help you, you just have to ask.
Consulting Services Find a company that specializes in medically necessary contact lens billing. Such companies may be able to guide you and your staff and train you on how to effectively bill for specialty contact lenses. While these consulting services may seem expensive, you must consider the amount of time that it would take for you and your staff to determine the nuances of each particular patient’s situation. What is your time worth?
When it comes to billing and coding contact lenses, a variety of high-quality resources are available. Sometimes it can seem overwhelming, but with the right help and the right tools, you can achieve success. CLS
REFERENCES
- GP Lens Institute. Codes for Medically Necessary Contact Lenses. Available at https://www.gpli.info/pdf/specialty-lens-codes.pdf . Accessed Oct. 5, 2021.
- Vicchrilli S. How to Use the New Contact Lens Codes and the New Femto Add-On Codes. EyeNet Magazine. 2012 Mar. Available at https://www.aao.org/eyenet/article/how-to-use-new-contact-lens-codes-new-femto-add-on . Accessed Oct. 5, 2021.