



The earliest scleral lenses were apical clearance or “fluid-filled.” These “sealed” lenses (identical to today’s modern scleral lens design) were used predominantly in managing irregular-shaped corneas. The scleral designs in the 1930s were “fluidless.” They were used for the correction of more regular refractive errors and required no “filling” solution; they used only a patient’s own tear film. The two fitting philosophies carried over with the widespread use of polymethyl methacrylate (PMMA) in the 1940s to 1960s. Interestingly, the history of the contact lens application solutions is as old as the lenses themselves and dates back to 1827, 60 years before the first contact lenses were ever made.
1827 John Hershel theorized that for a contact lens to perform on the eye, a transparent gelatin would be required to form a liquid lens between the lens and the cornea.
1887 Adolf Eugen Fick (the Father of Contact Lenses) suggested the use of a 2% grape sugar (glucose or dextrose) solution.
1892 Professor Henri Dor of France first suggested the use of physiologic saline as a lens application solution.
1926 Lewis Cooper used a 1.5% solution of baking soda and distilled water.
1937 Jacob B. Feldman, MD, suggested the use of a buffered saline solution that utilized a combination of sodium borate and boric acid solution as buffering agents.
Evolution of the Solution
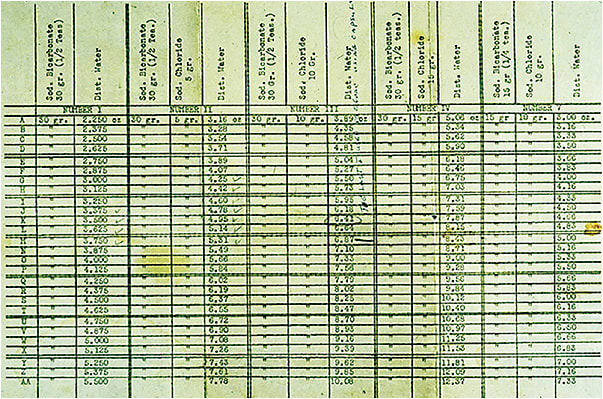
Practitioners recognized that no one solution was compatible for all patients. So, they began experimenting with ingredients such as different sodium chloride concentrations in conjunction with sodium borate, sodium carbonate, sodium bicarbonate, disodium phosphate baking soda, and methycel (Figure 1). Other experimental ingredients included glucose, glycerine, polyvinyl alcohol, gelatin, egg white, sea water, placental jelly, human blood serum, caster oil, mineral oil, and urea.
Throughout the early years of scleral lenses, practitioners searched for the correct concentration of buffered saline to extend patients’ wearing time and to reduce the presence of Sattler’s veil (corneal edema). At that time, the only method to reduce edema was “steeping-up,” in which a saline solution with a 1% sodium bicarbonate buffer was used to fill the lens bowl prior to application. At the start of the corneal clouding, lenses were removed and refilled with a 2% sodium bicarbonate solution. And, when the symptoms were about to start again, a 3% solution was used.
In the 1950s, there were two commercially available solutions in the United States in the form of premeasured sodium bicarbonate tablets that were dissolved in physiologic saline solution. These solutions were manufactured and distributed by Obrig Laboratories Inc. and House of Vision Laboratories (Figure 2). What a humble start to what would eventually become a multibillon-dollar-per-year industry. CLS
