



The refractive definition of myopia is the spherical equivalence of –0.50D or greater; high myopia is –6.00D or greater upon refraction (Weng et al, 2011). Myopia is also defined as having axial length greater than 24mm; high myopia is an axial length of 26mm or greater (Weng et al, 2011). A myopic refraction at an early age may increase, rapidly progressing into early adulthood (Morgan et al, 2012). High myopia is associated with sight-threatening ocular sequelae such as cataracts, retinal detachment, glaucoma, and choroidal detachment (Verkicharla et al, 2015). Because young myopic children are at greater risk for developing high myopia, it is important to prevent myopia progression as early as possible. Typical myopia control treatment options (mostly off-label) include soft multifocal lenses (Chamberlain et al, 2019), orthokeratology (Cho and Cheung, 2012), and low-dose atropine (Yam et al, 2019).
Using Multifocal Lenses
Myopia control through soft multifocals depends on focusing some light in front of the retina, which slows growth in axial length and retards myopia progression (Berntsen and Kramer, 2013; Kang et al, 2013; Ticak and Walline, 2013). Higher add powers may provide better myopia control, as they are able to focus light further in front of the retina compared to lower add powers (Rosén et al, 2012). To test this, the Bifocal Lenses In Nearsighted Kids (BLINK) study randomly assigned children to wear either commercially available single-vision contact lenses or medium- (+1.50D) or high-add (+2.50D) soft multifocal lenses for three years (Walline et al, 2020). The BLINK study included 294 children aged 7 to 11 years who had myopia ranging from –0.75D to –5.00D. This study demonstrated that treatment with high-add-power multifocals reduced the rate of myopia progression more effectively than did either the medium-add-power multifocal or single-vision lenses.
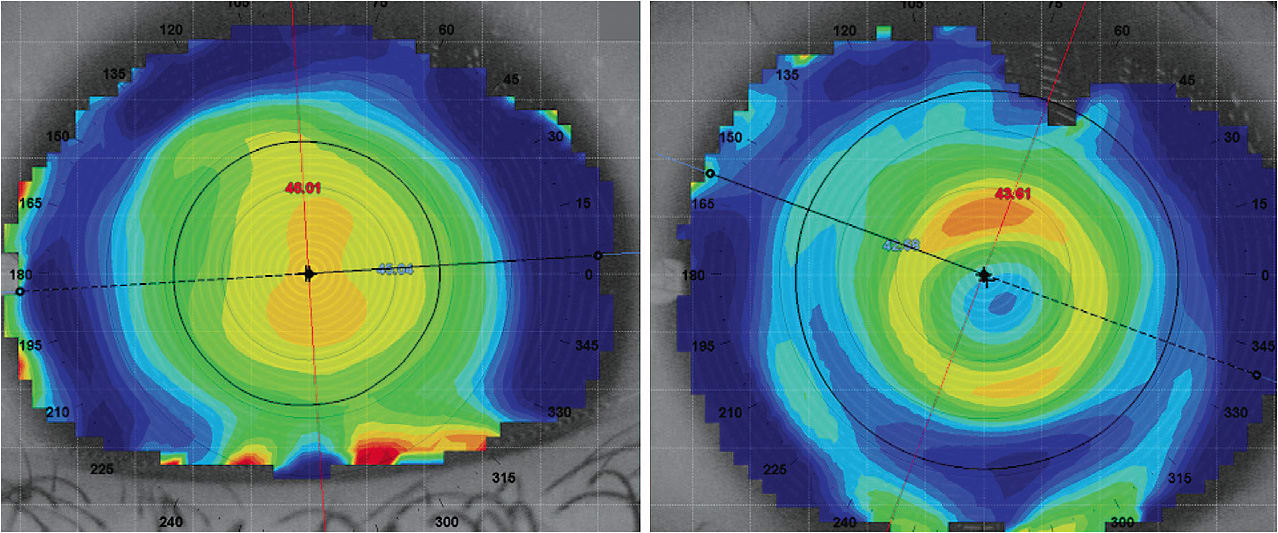
Therefore, when prescribing soft multifocals for myopia control, consider fitting children in higher add powers to decrease myopia progression. For example, an 11-year-old female who has progressive myopia was fitted into +2.00D add center-distance custom soft multifocal lenses in both eyes. Her manifest refraction and axial length were –5.25 –1.75 x 180 and 25.72mm OD and –4.75D and 26.12mm OS. Within one year, she had progressed to –6.00 –1.75 x 180 and 24.81mm OD and to –5.50D and 26.48mm OS. This patient was refitted into soft custom multifocal lenses with +4.00D add power (Figure 1). At the 18-month follow-up visit, she had not progressed refractively, and axial length progressed only 0.09mm and 0.17mm OD and OS, respectively. Despite the higher add power, she reported good quality of vision and was corrected to 20/20 in both eyes.
While no one option is best for every patient, soft multifocals have been proven effective especially when high add powers are used. CLS
For references, please visit www.clspectrum.com/references and click on document #303.