



A 35-year-old female came into the office for a comprehensive eye examination. She is a contact lens wearer and currently wears spherical daily disposables. She is a healthy individual but noted that she feels like her lens prescription probably needs to be updated, because she feels like she is not seeing things as well as she should be.
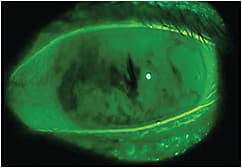
The power in her contact lenses is –3.00D for both eyes. Subjective refraction was OD –3.00D sph 20/20, OS –3.00D sph 20/20. Entrance tests and posterior segment evaluation were normal. Anterior segment examination revealed the following: lids/lashes—clear; Line of Marx—slightly irregular, with some anterior migration in both eyes; meibomian gland orifices—some capping in both eyes, with five-to-six meibomian glands yielding secretions per lid; conjunctiva—mild lissamine green staining nasally in both eyes; lid wiper—+1 lid wiper epitheliopathy; tear film breakup time—1 second in both eyes (Figure 1); and cornea—moderate inferior corneal staining.
During the pretesting process, the technician said that the patient needed to blink several times before readings with the auto-refractor could be acquired. Meibography demonstrated a +2 dropout. When the patient was questioned about any discomfort that she feels with her contact lenses, she responded: “Oh yeah, but that is just a part of wearing contact lenses.” When asked when she typically removes her lenses, she said “It is usually around 6 o’clock” (because that is when she feels that they “absolutely need to come out”). A matrix metalloproteinase-9 (MMP-9) test was performed and was positive in both eyes. A Standardized Patient Evaluation of Eye Dryness (SPEED) questionnaire was given, and the patient scored an 18.
It seems that there is more than meets the eye with this patient. Upon examining the clinical findings and hearing that she struggles with contact lens wear, it appears that dry eye disease is causing her vision problems. Additionally, the stability of the tear film was so poor that it was beginning to affect her vision. Interestingly, the comfort of her contact lenses was a secondary complaint that had to be extracted from her, because she viewed it as a necessary evil of wearing lenses.
The Treatment
This patient was prescribed a treatment plan that involved topical therapeutics, oral nutrition, and an in-office procedure; she was also refit into a contemporary daily disposable silicone hydrogel lens specifically designed to optimize ocular surface homeostasis. Over the next three months, she felt that her lens-wearing experience had significantly improved in both vision and comfort. She was surprised (and happy) that she didn’t have to change her prescription.
The Verdict
Dry eye disease is not only an ocular surface disease, it is also a vision condition. Understanding the influence that dry eye can have on a patient’s vision is critical. If blurry vision in contact lenses due to dry eye is the new normal, we don’t want to be normal. CLS