



Those of us who have been fitting scleral lenses for some time can probably agree that it can be a rewarding experience for both patients and fitters. Fortunately, in this day and age, there is a prolific amount of data and studies that speak to the benefits of treating corneal and ocular surface abnormalities with scleral lenses.
When it comes to the long-term effects of scleral lenses, there is still somewhat of a limited understanding of their impact on the ocular surface and the tear film. I found this to be the case when I was looking for information on conjunctival prolapse.
Conjunctival prolapse is an interesting finding in which forces under the lens cause the conjunctiva to be pulled over the limbus and peripheral cornea. While there is not much literature on this finding, we can still feel comfortable addressing it if we maintain a clear understanding of ocular anatomy and the overall design of scleral lenses.
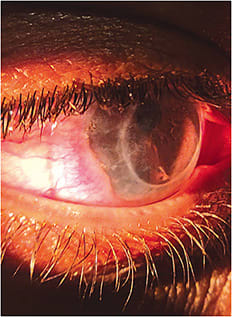
Figure 1 shows scleral lens-induced conjunctival prolapse occurring inferior-temporally. Slit lamp evaluation revealed excessive clearance in the peripheral/limbal area of the scleral lens. There was no change required within the overall sagittal depth or landing area. Decreasing the vault in the limbal area allowed me to realign the conjunctiva and to substantially reduce the hyperemia.
What the Studies Say
Looking for peer-reviewed information on the topic, I found a recent study (Fisher et al, 2021) that monitored 10 young, healthy adults who wore scleral lenses with varying amounts of lens fluid reservoir thickness for 90 minutes. Using optical coherence tomography, the researchers were able to quantify changes in the conjunctiva. The findings confirmed what we expected: conjunctival prolapse is more a function of limbal settling, not landing zone tissue compression or fluid reservoir thickness asymmetry.
While there isn’t much other historical data on this clinical finding, we need to be careful to not assume that it is completely benign (Caroline and André, 2013). Anecdotally, I can confirm that if left unaddressed, it can be difficult to readjust the alignment of the conjunctiva.
It is also safe to assume that the crowding within the limbal area will limit fluid exchange under the lens. Adequate fluid/tear exchange under a scleral lens is extremely important, because it helps maintain the ocular surface by providing oxygenated tears to the cornea and it removes debris, inflammatory cells, and metabolic byproducts that accumulate under the lens (Tse et al, 2019).
Fortunately, most labs give practitioners the ability to manipulate the limbal clearance area of the lens without affecting the central vault and the landing area. As more and more patients are being fit with this lens type, it’s important that we continue to challenge ourselves to provide our patients with the best wearing experience. CLS
For references, please visit www.clspectrum.com/references and click on document #316.