




AS THE EYE CHANGES with age, our patients may struggle with cataracts, dry eyes, endothelial cell loss, and corneal aberrations. Yet, despite some of these challenges, some of us embrace these changes and decide to correct presbyopia with contact lenses and even surgical treatments. Thankfully, we have access to amazing multifocal optics and customizable contact lens designs to successfully do just that.

Certainly, the ocular changes that occur with age have spurred the contact lens industry to improve technology and the patient experience with their contact lenses. Lens materials are more wettable and have a lower modulus, but provide adequate lens handling, and we see power expansions across all contact lens modalities in multifocal corrections.
The multifocal designs available are impressive and can offer the freedom from glasses that our patients are seeking. However, to properly prescribe these lens designs, we should understand some evaluation strategies and findings that can help us match a contact lens to each patient’s needs.
DESIGN BASICS
There are different ways to build the optics of a multifocal contact lens (Figure 1). Understanding the designs is certainly beneficial to prescribers, but adaptation and acceptance of the fitting process can also be improved by teaching the patient how the lenses work to provide the extended range of vision.
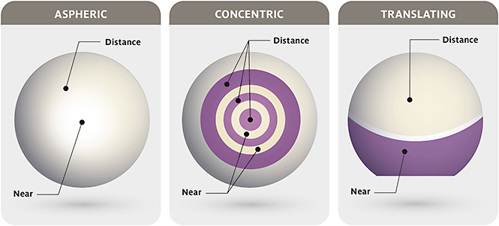
Aspheric lenses are a very common multifocal lens design. The lens powers are blended from far to near vision across the lens surface. Some designs hold the distance lens power at the center of the lens, called center-distance, while other designs are considered center-near. The gradual blending of near to far vision delivers both distance and near optics into the pupil at the same time, which creates a visual experience termed “simultaneous vision.” Explaining simultaneous vision to a patient that is new to multifocal optics can teach them why they may experience some reduced contrast sensitivity or some glare around light sources, which may encourage acceptance and eventual adaptation. Most soft multifocal contact lenses are center-near in design, whereas corneal GP multifocals are center-distance.
Concentric lenses are like aspheric designs in the way they deliver simultaneous vision to gain a wider range of functional vision. Concentric designs have distinct power rings rather than a gradual blend, and patients may comment that they see haloes around light sources. With the appropriate zone sizes and power prescriptions, patients can also adapt to these lenses quite well. With the advancements in today’s lens designs, many multifocals have both a concentric and an aspheric aspect, with a defined center zone surrounded by a blend of powers to take advantage of both design strategies.
The third multifocal contact lens design is exclusive to corneal GP lenses. This is the translating lens design, in which the multifocal optics are separated vertically through the lens, like a progressive or bifocal spectacle lens. The visual experience with a translating lens is called “alternating vision,” as the patient’s visual axis moves between the optical portion of the lens as the patient moves their eye.
These lenses perform best when they interact with both the upper and lower lids, so there can be some lens awareness that requires adaptation. However, because there is no simultaneous vision, vision is excellent once properly fit.
CUSTOMIZED APPROACH BASED ON REFRACTIVE ERROR
A positive first patient experience with multifocal optics can go a long way in the fitting process. Adjusting prescribing habits to match a patient’s routine visual experience is a good way to start in the right direction.
Patients who have little to no refractive error are often labeled as the toughest to fit in multifocal lenses, as they are accustomed to excellent vision quality and adaptation to simultaneous vision can be challenging. These patients will be more accepting of designs that have lower add powers or larger distance zones to begin with. It is important to keep the initial fitting simple and allow the patient to return to the clinic reporting which tasks they are succeeding at—or struggling with—to help guide the lens adjustments in small steps.
Myopic patients who prefer to take their glasses off to read can be just as challenging as our emmetropic patients. This patient group wants to gain near vision without losing their near vision quality. First diagnostic lenses should be biased toward near vision to show the patient that they can maintain their near vision and gain some distance acuity. An adjusted lens can add more distance by increasing the distance zone or modifying add power.
Patients who have high refractive errors are excellent candidates for multifocal contact lenses, as they are accustomed to not seeing well at distance or near, so providing good distance vision with some function at near will be welcomed by these patients.
PUPIL SIZE AND LENS OPTICS
Recognizing how pupil size affects the performance of optics is one of the foundational aspects of multifocal prescribing (Table 1). A pupil 3mm or less in diameter could be considered small, while a larger pupil would be around 4.5mm and greater.
| PUPIL SIZE | CHALLENGE | CENTER-NEAR TIPS | CENTER-DISTANCE TIPS |
| Small Pupil (< 3mm) | Place all usable optics inside pupil | Keep near zone small to maintain distance vision | Overprescribe add power to push near optics into pupil area |
| Large Pupil (> 4.5mm) | Maintain satisfactory image quality | Design near zone at 50% or less of pupil diameter | Start with large center zone and decrease with adaptation to improve near vision |
Patients who have small pupils have the benefit of an increased depth of focus; however, it can be a challenge for these patients to utilize the spread of optics across the lens surface. If the multifocal lens has a center-distance design, consider overprescribing the add power. This technique is used to push the desired add power of the contact lens closer to the center of the pupil.
If the center-distance zone size is modifiable, it can also be made smaller to allow some of the near optics to enter the peripheral pupil. If the lens has center-near multifocal optics, the central zone needs to be smaller in diameter, so that the patient is also able to use the peripheral distance optics. Patients who have small pupils tend to have good vision quality in multifocal contact lenses, but they can struggle with a limited range of vision.
Conversely, patients who have larger pupils can often utilize the entire optical design of the lens, but it can be a challenge to maintain good vision quality. The peripheral light rays entering the peripheral pupil can create glare, haloes, and other visual aberrations. If the contact lens is a center-distance design, consider increasing the distance zone to maintain distance quality.
These patients may also need more coaching and adaptation time, so consider starting with a low-medium add power to encourage adaptation and increase add power over time to control aberrations. Center-near contact lens designs should be kept at 50% or less of the pupil size to ensure that the patient can continue to comfortably see at distance.
AN IDEAL FIT
It’s easy to assume that we’re only talking about GP lenses when discussing customized fits. However, in my practice, most patients who are seeking an improved lens wearing experience are wearing soft contact lenses. Custom soft lens designs are an excellent way to build your practice without having to invest in numerous fitting sets or additional technology.
A basic corneal topographer will assist you with your custom soft lens design, so this is preferable to autokeratometry. A topographer can tell you about a patient’s horizontal visible iris diameter (HVID), corneal eccentricity, keratometry readings, pupil size, and the position of the visual axis. All these parameters play a role in choosing an ideally fitting soft contact lens, especially if multifocal optics are desired.
The relationship between contact lens base curve and corneal curvature has been a foundational topic for many years. However, in the case of soft contact lenses made from modern materials, the correlation between corneal diameter and contact lens sagittal depth is the more impactful fitting relationship. Larger corneal diameters will create a deep sagittal depth, requiring a larger and, therefore, deeper contact lens to properly align and center on the cornea. The primary determinants of corneal sagittal depth, in order of most influence, are HVID, corneal eccentricity, and corneal curvature.
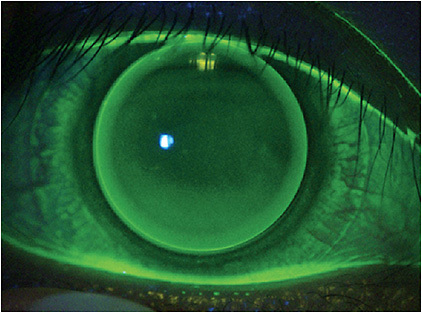
When assessing corneal GP lenses, patients who already wear aligned and centered lenses are the best candidates for GP multifocals; however, even lenses that are moderately lid attached can be successful in a multifocal design with proper knowledge of the multifocal design and/or guidance from laboratory consultation. Ideal aspheric corneal GP multifocals are centered on the cornea, with a small amount of movement with each blink (Figure 2). They should also translate slightly with downgaze to allow the pupil to move into the peripheral optics of the lens where higher add powers are located.
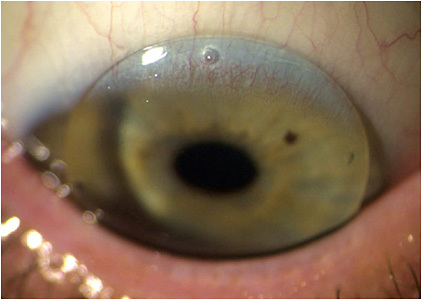
In general, a stable fit is achieved by modifying the diameter and peripheral curves. Most of the troubleshooting involves power and zone size adjustments. Translating GP lenses should provide quick, limited movements in primary gaze, keeping most of the pupil in the top half of the lens. They should interact with the lower lids on down gaze to provide translation of the lens across the superior limbus to ensure that the pupil moves into the segment of add power (Figure 3).
Translating lenses use different techniques to improve centering and decrease lens movement compared to aspheric lenses. In many cases, decreasing the diameter of a translating lens will limit interaction with the lids and create a more stable fit. Ultimately, each multifocal has its design nuances, and the laboratory consultant is a valuable resource to optimize the lens.
Scleral and hybrid lenses are approached similarly to soft aspheric lens designs, as the lenses are fit stable to the eye with minimal to no movement. However, most of these lenses have customizable zone sizes and add powers, which can increase performance compared to soft multifocal lenses.
Lastly, an over-refraction can also assist in understanding how the lens is fitting to the eye. Expected over-refractions are going to be between –0.50D and +0.50D to improve distance vision. If a larger, unexpected over-refraction is obtained (e.g., –2.00D), this demonstrates that the patient is looking through the near portion of the lens and the distance optics are not being utilized. This finding would warrant a zone size or design change rather than a power change.
The same process can be used for add power refinements. If the patient needs full plus to read (e.g., +2.00D), it shows that the patient is looking through the distance portion of the lens rather than the add. A helpful tool in these cases is a topography over the contact lens, the image where the lens optics are in relation to the visual axis and how the zone size compares to pupil size.
PREMIUM VISION EXPERIENCES
Sometimes, no matter what the power or zone size adjustment is, the patient continues to struggle to see well. An over-topography is an excellent troubleshooting tool to ensure our patients are getting the best visual experience possible.
As the optics of a multifocal lens are typically on the front surface of a contact lens, a topographer can image the location and zone size of the lens optics compared to the patient’s visual axis and pupil size. If the multifocal optics are found to be misaligned from the visual axis (Figure 4), many custom designs can decenter the multifocal optics to better align the distance and near zones in the patient’s vision.
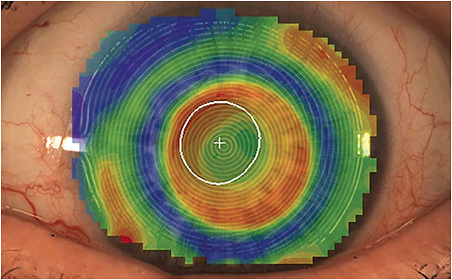
If the lens requires decentering of optics (Figure 5), the laboratory consultant will ask for the distance and angular direction to which the optics need to be moved. The topographer will center the scan over the patient’s line of sight, and an outline of the multifocal optics can be drawn. The system can then calculate the distance in millimeters and the direction from the patient’s line of sight to the center of the multifocal.
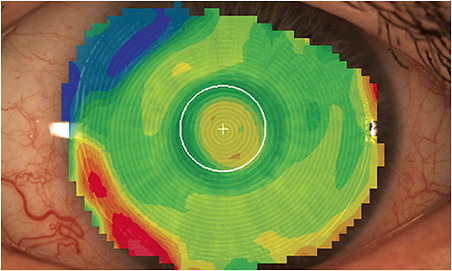
FIGURE 5. This image shows the results after decentering the optics on the scleral lens from Figure 4.
Contact lens technology is also advancing in the correction of higher-order aberrations. This requires an extremely stable lens fit, but it just might be the holy grail of multifocals. Stay tuned for more information on this exciting development.
SUMMARY OF SURGICAL OPTIONS
Our knowledge of multifocal contact lenses makes us excellent resources for our patients when they have cataract surgery. The following points may be helpful in counseling our patients who wear multifocal contact lenses and hope to continue to succeed with multifocal optics after intraocular lens (IOL) implantation (Table 2).
| IOL TYPE | PROS OF DESIGN | POTENTIAL CHALLENGES |
| Trifocal/Multifocal | Excellent range of clear vision, even greater than multifocal contact lenses | Haloes around light source, tend to improve with adaptation |
| Extended Depth of Focus | Fewer haloes compared to trifocal | Near vision can be good in patients who have smaller pupils; however, some patients require frequent use of reading glasses |
| Standard Monofocal | Great vision quality after correction of residual refractive error with glasses or contact lenses | Patients will require a contact lens refit after cataract surgery |
Speaking from personal experience, patients who use multifocal contact lenses do quite well with multifocal implants. These IOLs are known to create some visual haloes; however, patients using multifocal contact lenses adapt quite quickly and really enjoy their “cataract-free” vision quality. Patients who have slightly irregular corneas from a corneal condition or long-term GP lens wear may not be great candidates, as the corneal optics need to be free from higher-order aberrations for the IOL to perform best.
THE FINISH LINE
There are many aspects of a custom multifocal lens that can be modified, and sometimes it can be difficult to know when to complete a lens fitting. My obligation as a contact lens prescriber is to provide the best optics possible while maintaining corneal health. Thankfully, with the advancements in technology in contact lens manufacturing, and our in-office diagnostics, we can usually meet the goals of the patient, and our obligations as providers. CLS