



ONE STRUGGLE that all contact lens fitters have is the struggle to get lenses to center. There is the large decentration that comes with a grossly bad fit, and then there is the mild decentration that occurs because a patient’s corneal apex is slightly decentered. The latter is far more challenging to fix, even though it is a “smaller” issue.
When practitioners are doing orthokeratology (ortho-k) for myopia management cases, this problem may not be as important. For patients who are younger, crisp, clear vision may be less of a concern. They may not notice glare or halo as much as an adult wearing ortho-k lenses with slight decentration will. But recent evidence has come out that may shed some light on a small advantage to having a decentered lens.
A retrospective analysis was done on 352 children who had been doing ortho-k for myopia management (Lin et al, 2021). Their axial length was measured at the start of the study and then again at the 12-month mark. The children in the study who had smaller treatment zone sizes and larger treatment zone decentration had the least progression in their myopia. The study noted that children who had larger decentration were associated with smaller axial elongation.
However, the authors of the study did not suggest doing a deliberate decentration, as it could lead to visual discomfort, ghosting, and visual fatigue. In my clinical experience, children tend to do extremely well even when a lens is slightly decentered.
How many times have children come into the office with 20/50 vision because they failed a vision screening test? The children had not complained, and some parents might not have even noticed that their child wasn’t seeing well. It isn’t until children are shown what clarity of vision could be that they begin to demand better vision.
Many of these children do very well when their refraction is corrected in a portion of their visual axis. Children often deal very well with multifocal lenses and ortho-k in situations in which adults would struggle. They also do very well with atropine and slightly dilated pupils when an adult would struggle. Remember that children are not just tiny adults; their visual function is different from that of adults.
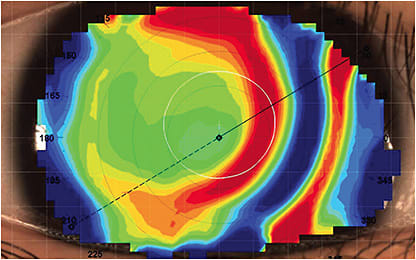
Clinically, the aforementioned publication provided relief. When seeing an ortho-k patient who has suitable visual acuity and visual function but has some decentration, I have historically tried to solve this fit problem. Many times, this leads to multiple visits that result in minimal visual improvement (which the child may not notice). Now, topography could possibly help (Figure 1). Some decentration may be protective for the progression of myopia, and when the child is satisfied with his or her vision, the topography should be left alone (Lin et al, 2021).
So, in the future, if your ortho-k is a little off, you may be right on! CLS
References
- Lin W, Li N, Gu T, et al. The treatment zone size and its decentration influence axial elongation in children with orthokeratology treatment. BMC Ophthalmol. 2021 Oct 12;21:262.