




The 2024 GLOBAL SPECIALTY LENS SYMPOSIUM (GSLS), presented by Contact Lens Spectrum, was held Jan. 17-20 at Horseshoe Las Vegas. This year’s program, with close to 1,000 in attendance, focused on the theme of innovation across all aspects of specialty lenses.
The schedule included four workshops (one was presented in English and Spanish), nine general sessions, and 18 breakouts with an emphasis on keratoconus, myopia, artificial intelligence, scleral lenses, imaging, orthokeratology (ortho-k), and more. In addition, there were 140 scientific posters, five free papers highlighting cutting-edge research, eight rapid-fire poster talks, and 45 sponsored presentations, allowing attendees to learn about new specialty lens designs, technologies, and services.
The 2024 GSLS Education Committee is comprised of Jason J. Nichols, OD, MPH, PhD (chair); Karen DeLoss, OD (vice chair); Patrick Caroline; Eef van der Worp, BOptom, PhD; and Ashley Wallace-Tucker, OD.
Here, we offer some highlights from eight of the nine general sessions. For a recap of the keynote speech, see “Contact Lens Wear Is Intrinsically Inflammatory.”
THE GREAT DEBATE 2.0
After the keynote, Loretta Szczotka-Flynn, OD, PhD, moderated a spirited debate between Nathan Efron, AC, PhD, DSc, and Edward S. Bennett, OD, MSEd, on the topic of soft versus GP contact lenses. Professor Efron began by arguing that GP lenses are virtually extinct. However, he did add a caveat that while GPs are on life support for regular refractive correction, they are still being used in certain specialty circumstances.
In arguing that GP lenses are still alive, Dr. Bennett pointed out several instances in which Professor Efron predicted the obsolescence of GPs (by 1994 and then by 2010) and then writing their obituary in 2010. However, Dr. Bennett also pointed out that a recent International Contact Lens Prescribing Survey noted that GP lenses have exhibited continuous growth between 2009 and 2022.1
Other topics of debate included whether rigid lenses should only be taught at the postgraduate level, whether rigid lenses are a healthier (safer) option compared with soft lenses, whether ortho-k is worth the effort, and whether rigid GP lenses provide better vision and more refractive options than soft.

KERATOCONUS: PAST AND PRESENT
The general session titled “Keratoconus: Research of the Past and Clinical Indications for the Future” included clinical pearls from many of the leading experts in this area. Dr. Szczotka-Flynn presented the results of three studies which, over time, showed the changes in contact lens correction modalities in keratoconus, notably in the introduction and increasing usage of scleral lenses2-4 (Table 1). Highly correlated factors for keratoconus include hay fever and allergies (53%)3 and eye rubbing in nearly half of all individuals who have keratoconus.2,5
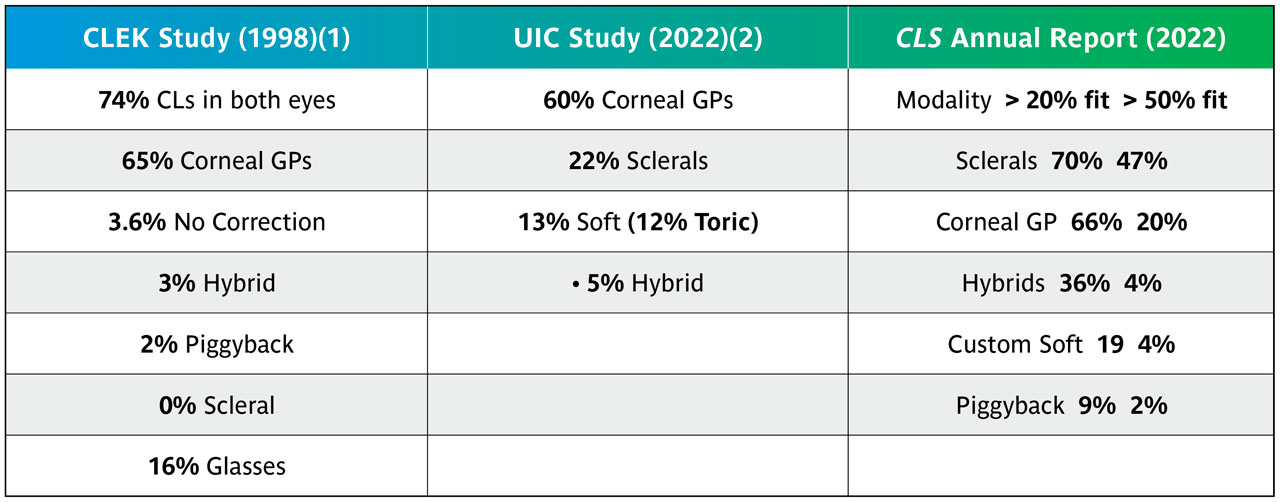
The question of whether keratoconus is inherited is more difficult to answer. In the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) study, 13.5% reported a family history, whereas other studies demonstrated a higher odds ratio of inheritance as a risk factor.5,6
Jeff Sonsino, OD, addressed the benefits of technology, particularly as it pertains to scleral lenses. Although the audience, when polled, still preferred corneal GPs as their “go-to” lenses, it is evident that the standard of care for the management of keratoconus is shifting toward scleral lenses.
Dr. Sonsino emphasized the benefits of both scleral topography as a great technology for accelerating the fitting process and wavefront technology. He performs wavefront aberrometry on every scleral lens, and wavefront aberrometers typically tell practitioners the breakdown between higher-order aberrations (HOAs) and lower-order aberrations (LOAs). This is clinically relevant because if HOAs are above 1D, you can expect diminished visual acuity or subjective clarity, even when a sphero-cylindrical power is corrected on the front surface of a scleral lens.
Most patients have an acceptable result when correcting LOAs. If HOAs are high, it is important to use an HOA-correcting lens. Non-wetting can be a problem with these lenses; therefore, using a polyethylene glycol (PEG) coating is important.
Jan Bergmanson, OD, PhD, addressed corneal cross-linking for young patients. He emphasized that cross-linking should be performed after a diagnosis of keratoconus has been confirmed. When a young person is diagnosed with keratoconus, the practitioner should recheck keratometry/topography values and pachometry after three and six months, as progression will not be more accelerated than that. A cautious approach to treatment is recommended.
RAPID-FIRE POSTERS
This year, more than 140 posters were submitted. See the winners of this year’s contest below. In addition, the judges chose eight submissions to be featured in a rapid fire-style presentation of the findings.
“OC-SAG values in 360 degrees” – Javier Rojas-Viñuela, OD, MSc; Eef van der Worp, BOptom, PhD; and David Piñero, PhD In this study, Dr. Rojas-Viñuela and colleagues analyzed 50 healthy eyes with profilometry and obtained sagittal height of the anterior eye (OC-SAG) values for 15mm and 12.8mm in 1º steps. They then compared those data to a historical database of another group of 39 patients. A three-dimensional model of mean OC-SAG values in the 360º was also built and compared with the profilometry and the anterior segment optical coherence tomography (AS-OCT). He noted that common patterns were shown in the three-dimensional models. However, additional research will be needed to determine if the data is clinically significant.
“Welcome to the Hybrid Club: Fitting Hybrid lenses on Eyes with Keratoprosthesis” – Calisandra Larson, OD Dr. Larson told the case of a 38-year-old female who presented for a contact lens fitting in the setting of keratoprosthesis following a failed penetrating keratoplasty. The patient’s history included a fishhook injury to the eye when she was 11 years old. She detailed a series of treatments and procedures that the patient has had since then. Dr. Larson noted that the goals of a contact lens fit were to minimize lens interaction with a glaucoma shunt, improve patient visual quality, and prevent corneal melt. She ultimately dispensed a hybrid lens and achieved a best-corrected visual acuity of 20/25 with no interaction with the shunt.
“The Relation Between Overnight Orthokeratology Lens Decentration and Axial Elongation” – Mark Bullimore, MCOptom, PhD; Jackson Lau, OD; and Maria Liu, OD, PhD, MPH, MBA Dr. Bullimore performed a literature search for “orthokeratology and myopi*” and (axial or elong*) that was not a review or meta study. Of the 526 articles screened, 40 included axial elongation data for children and seven examined the relationship between lens decentration and axial elongation. He noted that all studies found increased lens decentration was associated with slower axial elongation. He suggested that while practitioners shouldn’t intentionally decenter the lens, they should aim to get the plus power closer to that area.
“Customizing Multifocal Scleral Lenses into a Myopia Treatment Option” – Nina Wang, OD, and David Kading, OD Dr. Wang presented a case report of a 14-year-old female who started myopia management treatment at the clinic when she was 7 years old. The patient had previously tried soft, multifocal, ortho-k, and multifocal GP lenses. Ultimately, she had success with atropine and a scleral lens.
“Split Prism Wavefront Guided Scleral Lenses to Resolve Vertical Diplopia and Improve Aniseikonia-like Symptoms” – Becky Su, OD; David Slater; Nicholas Brown, BS; Steven Greenstein, MD; Peter S. Hersh, MD; and John D. Gelles, OD Dr. Su presented a case study of a 56-year-old male with myopia and a right hypertropia who reported visual discomfort and an aniseikonia-like “coke bottle” visual distortion in the right eye with prism-incorporated spectacles. He was initially fit with a prism incorporated scleral lens (pSL) with 3pd of vertical prism split to correct the diplopia, but the aniseikonia-like symptoms persisted. Then, a prism-incorporated wavefront-guided scleral lens (pwfgSL) was created for his right eye only in an attempt to balance the visual quality. Dr. Su noted that the use of pwfgSLs OD and pSL OS for this patient was effective in managing both diplopia and aniseikonia-like symptoms.
“Sweet Dream, Sweet Dreams Dry Eyes, a Case of Overnight Scleral Lens Wear” – Jina Chong, OD; Chi Nguyen, OD, Patrick Caroline; Matthew Lampa, OD; Randy Kojima; and Mari Fujimoto, OD In this case study presented by Dr. Chong, a 33-year-old male had a history of radiation therapy for leukemia. He previously underwent dry eye treatments. Comanagement with the corneal specialist led a diagnosis of graft-versus-host disease (GVHD). Initially, he was fit and successful with a scleral lens for daytime wear but still experienced overnight corneal erosions. He was subsequently fit for overnight scleral lens wear. Dr. Chong and colleagues concluded that scleral lenses can be used to correct difficult refractive errors and rehabilitate the epithelium when traditional dry eye therapies are ineffective.
“Innovating Optometric Education: A Comprehensive Approach to RGP Contact Lens Teaching and Learning” – Jimmy Sung Hei Tse, Angel C.K. Wong, Dorothy S.M. Chung, Cherie Y.K. So, Ken K. Wan, and Thomas C. Lam Mr. Tse noted that current optometry students acquire their rigid lens knowledge through lectures and clinical practices, which is a very peer-dependent model as they can’t try out too many lenses on a single subject’s eye. He also explained that performing simulated fits isn’t the same as actual fittings. He then described an interactive web-based rigid lens learning platform from Hong Kong Polytehnic in which students can watch a video that depicts their fitting choice. They are then able to choose a different option and see how that one would work out. In this study, two quizzes on lens-fitting grading using recorded videos were given to students following didactic teaching, with and without platform use. The researchers concluded that the platform was an effective tool in rigid lens teaching and learning.
“Two curves is better than one: Management of post-refractive myopia with a novel custom-soft dual base curve lens design” – Sheila Morrison, OD, MSc; Alia Cappellani, OD; Vanessa Lin, OD; and Andrea Lasby, OD Dr. Morrison explained that fitting traditional soft contact lenses is complicated on post-refractive corneas due to central flattening. In this study, a novel custom silicone hydrogel lens was augmented with a flatter central base curve (BC) and a steeper peripheral BC to provide a more optimal fit for individuals who have post-refractive corneal shape while remaining in a more common contact lens modality. In this case series, the novel dual BC soft contact lens design demonstrated the possibility to fit the oblate shaped cornea without excessive central clearance and land adequately in the periphery for acceptable lens movement. Dr. Morrison noted that multifocal and toric options will be needed to further explore the clinical use of dual BC soft lenses, because they may be less forgiving than single-vision powers with lens flexure.
REGULATORY, ETHICAL, AND FDA ISSUES
Craig Norman moderated “Insights into the Contact Lens Industry: A Panel Discussion of Regulatory, Ethical, and [Food and Drug Administration (FDA)] Issues.” Panelists Mark Bullimore, MCOptom, PhD; Katie Gilbert-Spear, OD, JD, MPH; Ashley Wallace-Tucker, OD; and Bret Andre, MS, detailed concerns and considerations from the perspectives of a researcher, a clinician, an attorney, and a regulatory specialist.
For example, Dr. Wallace-Tucker presented the case of a 22-year-old noncompliant male who is overusing his daily disposable lenses and sleeping in them as well. The practitioner is also treating his family. She asked what practitioners should do in this case. Drs. Wallace-Tucker and Spear advised documentation. Dr. Bullimore suggested getting the patient to sign a “contract” of some sort and determining if and when one should discharge the patient for noncompliance. Craig Norman also noted that there are various levels of noncompliance.
Next, Dr. Spear discussed informed consent. She noted that for a proper informed consent, the provider educates the patient about the risks, benefits, and alternatives of a given procedure or intervention; the patient is allowed to ask questions and receive answers; he or she is given sufficient time to decide if they want to consent; and the patient communicates verbally and in writing that they understand. Dr. Spear said this should be part of a standard workup, but practitioners may need to obtain an additional consent for a specific lens or treatment that is not normally done. Dr. Bullimore added that informed consent is a process; it is not just filling in a form.
In light of recent issues with some eye drops, another notable topic was adverse event reporting. Dr. Bullimore noted that there is a voluntary adverse event reporting program for patients and practitioners, but that manufacturers have a mandatory obligation to report any issues. When he asked who in the audience had ever reported, only two hands went up. Mr. Andre noted that practitioners can report events to the manufacturer instead of the FDA.
Other interesting discussions included off-label product use, conflict of interest, and product recall and safety alerts.
SPECIALTY CONTACT LENSES
Many types of specialty lenses were discussed in the “Contemporary Topics in Specialty Contact Lenses” session. Daddi Fadel, DOptom, talked about the importance of scleral lenses in special populations. She emphasized that scleral lenses are beneficial for all populations, with no limits on age. Common challenges with young children and the elderly are hygiene and compliance, handling issues, and the need for a caregiver to be present at visits and to assist with care and lens costs. It is important to talk in a language that they can understand and allow extra time for patient education.
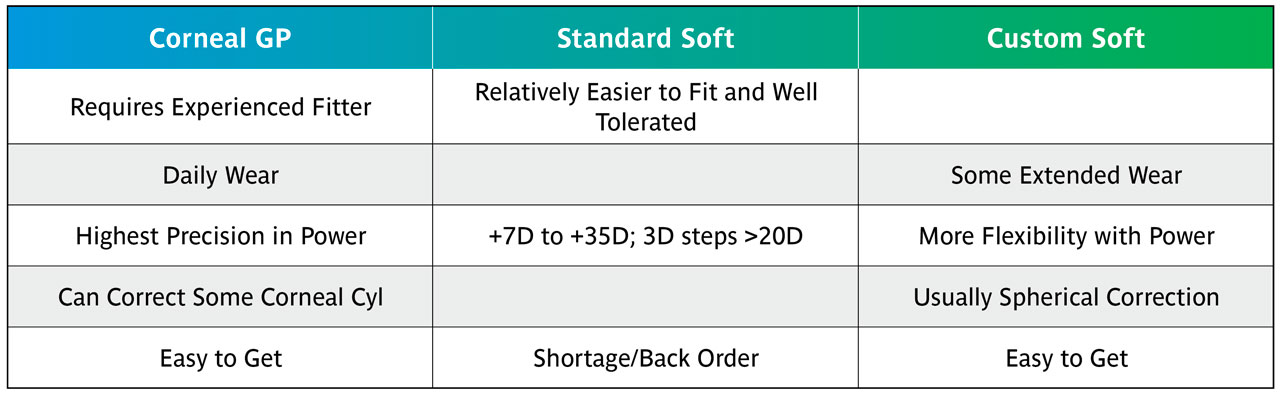
In “Pediatric Aphakia and Trauma in Youth,” Sheila Morrison, OD, MS, reviewed her clinical guidelines for corneal GP, standard soft, and custom soft lenses (Table 2). She offered the following recommendations: market your services for kids and contact lenses; become a referral site; comanagement may come with challenges; set a fee structure for services and products; and use staff effectively.
Philippe Seira reported on the topic of “Patient and Parent Communication for Myopia Management.” Results of his in-house study of 101 people with an average age of 15, which ran from September 2022 to August 2023, showed that 46% were fit with ortho-k, 12% with soft myopia control lenses, 9% with myopia control glasses, and 14% with customary glasses or contact lenses; and 19% discontinued/abandoned myopia management. He concluded with the following recommendations:
1. Have a good knowledge of the available products.
2. Enjoy working with children and their parents.
3. Develop your own communication tools.
4. Develop your own methods to achieve good results.
5. Ensure good compliance.
Boris Severinsky, OD, presented on “Scleral Lens Use in Ocular Cicatricial Pemphigoid (OCP).” In the results of his Emory University study with a mean follow-up of approximately 18 months, about 90% of patients were successful with scleral lenses.7 Keratopathy grades improved in all fitted patients. There was no progression of symblepharon or fornix shortening.
Subjective ocular comfort grading also improved in all patients and the overall vision improved from an average of 20/80 to 20/30. The bottom line was that scleral lenses provide ocular surface protection, hydration, and nourishment for the OCP patient, improving ocular health and comfort while enhancing vision and overall quality of life.
Steve Sorkin, OD, presented on “Suture Related Complications.” He indicated that sutures should be removed if they are broken, loose, exposed, or vascularized. It is always important to utilize fluorescein in evaluating sutures. If staining is observed, you must investigate for a loose, broken, or exposed suture. Sutures should not be removed when there is 1) an abscess/infection; you will need to culture first; 2) a recent surgery with destabilized wounds; or 3) anterior chamber reaction/hypopyon.
FREE PAPERS
In this year’s Free Papers section, attendees listened to snapshots from five papers.
Kishan Patel, OD, presented on the creation of a new clinical grading scale to evaluate scarring in keratoconus patients. In this study, 14 patients (14 eyes) with and without existing scarring due to keratoconus had corneal transparency grading on a five-point scaling system. Dr. Patel noted that the location and density of scars are important factors affecting visual acuity.
In his presentation, Randy Kojima looked at elevation data. He noted that a tool can increase fit success because practitioners will be able to see how a lens will lift. He noted that practitioners can then adapt the lens and customize per quadrant.
Evan Elam, OD, spoke on a novel method of lens prescription and manufacture, which will allow wavefront correction to be applied to any commercial scleral or soft contact lens, aligning wavefront-guided lens practice with clinical norms. He found that the novel method of manufacture does not induce variability in the manufacturing process beyond what is already observed in the established method of manufacture.
Dr. Fadel looked at the use of scleral lenses to manage dry eye symptoms in habitual soft lens wearers. Specifically, she examined whether coated or uncoated sclerals would be more beneficial (in improving ocular comfort and reducing dryness) in symptomatic soft lens wearers. She found that switching symptomatic soft lens wearers to scleral lenses improved comfort and reduced dryness symptoms after one month of wear, with little reduction in ease of lens handling.
Langis Michaud, OD, MS, presented results of a study that aimed to confirm the symmetry of axial length in relation to refraction in the peripheral retina; a second study measured the response to strong myopic defocus stimuli at various angles from the macula, using electroretinography. He found that the symmetry of the axial length, which is lost beyond 20º, would help to understand why such a limit exists. Dr. Michaud noted that the results show that the amplitude of the direct wave, caused mainly by photoreceptors and bipolar cells, is not influenced by the design of the lenses.
The amplitude of the induced wave, however, is significantly decreased when a lens with a smaller optical zone is worn, causing defocus over a larger area. Dr. Michaud explained that this significant difference only concerns an area that corresponds to a retinal eccentricity of 15.7o to 24.0o. He said that this implies that this area is likely the most sensitive to myopic defocus.

SCLERALS, SCLERALS, SCLERALS
Always a very popular general session at GSLS, “Using Technology to Maintain Ocular Health in Scleral Lens Wear” was again very informative. Greg DeNaeyer, OD, discussed advancements in scleral technologies including GP materials, surface treatments, soft lens use with scleral lenses, scleral lens filling solutions, and scleral shape and design. He concluded that there are several areas of concern, including corneal edema.
Hyper-Dk materials should be used to reduce oxygen stress accompanied by a low fluid reservoir to optimize oxygen transmission. Michaud and colleagues have recommended a > 150 Dk material, ≤ 250-micron center thickness, and ≤ 200-micron central clearance.8 Other options could include a corneal GP lens or a partial thickness corneal transplant followed by a scleral lens fitting.
Mile Brujic, OD, presented on the topic of “Using Technology to Maintain Ocular Health in Scleral Lens Wear Anterior Segment OCT.” He found that using the OCT is a much better method of estimating scleral lens clearance than observation.9 Optimal limbal clearance of 100 to 200 microns and 50 to 100 microns is acceptable.10,11 The use of vertical OCT scans is valuable, as any inferior decentration of a scleral lens can result in a greater tear reservoir inferiorly and potentially greater corneal swelling. His bottom-line recommendations included creating a process in the office for utilizing AS-OCT for scleral lenses; measuring the corneal thickness along with epithelial thickness; and assuring appropriate central and limbal clearance as well as an appropriate landing zone.
Dr. Bergmanson presented on the effect of scleral lens wear on intraocular pressure (IOP). He showed that Charles McMonnies, DSc, had originally hypothesized that several factors combined to create a negative suction of the scleral lens onto the eye, resulting in elevated pressure.12 Since then, a number of studies utilizing anterior segment evaluation techniques have resulted in varying results but no consensus.
Recently, Walker and colleagues13 evaluated IOP and optic nerve head morphology during scleral lens wear and found using this technology that scleral lenses had minimal effect on IOP. Dr. Bergmanson’s bottom-line recommendation was that we have been using the wrong technology and need to concentrate on posterior segment technology.
In “Using Technology to Maintain Ocular Health in Scleral Lens Wear,” Gloria Chiu, OD, discussed the different conditions and their management, as well as advanced techniques to optimize design and vision, such as cutout notches, peripheral vaults, channels, fenestrations, HOA correction, decentered optics, and multifocal designs. She also presented a great source for scleral lens fitting tips and tricks.14 Her bottom line was that we cannot ensure the best scleral lens fit and design with technology alone. We must also understand the ocular surface, treat each patient individually, and use technology to monitor changes over time.
MYOPIA MANAGEMENT
A fascinating peek into the future was presented in the “Top Technology to Crack the Myopia Code” general session. Foo Li Lian, MD, presented a comprehensive review of the literature as it pertains to the effectiveness and application of low-dose atropine. One must take into consideration the patient’s lifestyle, their ability to wear contact lenses, their acceptance of glasses, and the possibility of atropine allergy. The treatment should be personalized based upon patient data, progression, and risk-benefit prior to making the decision.
Dr. Bullimore presented on “Axial Length in Myopia Management.” The major question that he addressed was: “Which is more important: Refractive error or axial length?” Axial length is more important than refractive error in disease association, does not require cycloplegia, and is relatively more sensitive, and treatment can influence optics independently of axial length. Whereas refractive error is beneficial in diagnosing myopia, the best way to monitor progression is to measure axial length. He concluded that although refractive error has value and will continue to be important clinically, axial elongation is the gold standard for assessing myopia control from an evidence-based perspective.
Certainly one of the most interesting and futuristic myopia talks was given by Vishakha Thakrar, OD, titled “Finally! Myopia Management Glasses.” The presenter has had extensive experience with various contemporary myopia management spectacles and presented the different types currently in use. Dr. Thakrar indicated that the landscape has changed completely due to the newest generation of spectacles with this ability.
Dr. Thakrar reported on four separate studies in which both refractive error progression and axial length change were significantly less in those wearing the glasses than in the control group.15-18 The effect is even greater if combined with low-dose atropine.19 She stated that myopia management glasses have become invaluable to her practice.
The session concluded with a presentation by Richard Wu, OD, MS, titled: “Optimize Your Orthokeratology Corneal Topography for Myopia Control.” He emphasized the importance of corneal topography in evaluating ortho-k patients, beginning with capturing a good image. It is important to look at the treatment zone profile; the more of the treatment zone that lies within the pupil, the more myopia reduction is possible. In a post-ortho-k corneal topography map, it is important to observe the location of the apex, the defocus amount, and the treatment zone diameter and shape in order to optimize myopia control.
REFERENCES
1. Morgan PB, Woods CA, Tranoudis IG, et al. International Contact Lens Prescribing in 2022. Contact Lens Spectrum. 2023 Jan;39:28-35.
2. Zadnik K, Barr JT, Edrington TB, et al. Baseline findings in the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study. Invest Ophthalmol Vis Sci. 1998 Dec;39:2537-2546.
3. Scanzera AC, Deeley M, Joslin C, McMahon TT, Shorter E. Contact Lens Prescribing Trends for Keratoconus at an Academic Medical Center; Increased Utilization of Scleral Lenses For Severe Disease. Eye Contact Lens. 2022 Feb 1;48:58-62.
4. Bennett ES. 2022 GP and Custom Soft Annual Report. Contact Lens Spectrum. 2022 Oct;37:24-31.
5. Hashemi H, Heydarian S, Hooshmand E, et al. The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea. 2020 Feb;39:263-270.
6. Almusawi LA, Hamied FM. Risk Factors for Development of Keratoconus: A Matched Pair Case-Control Study. Clin Ophthalmol. 2021 Aug 16;15:3473-3479.
7. Severinsky B. Contact lens use in ocular cicatricial pemphigoid. Presented at the 49th European Contact Lens Society of Ophthalmologists. 2022 Sept. Paris, France.
8. Michaud L, van der Worp E, Warde R, Giasson CJ. Predicting estimates of oxygen transmissibility for scleral lenses. Cont Lens Anterior Eye. 2012 Dec;35:266-271.
9. Brujic M. Estimating scleral lens clearance and comparing it to OCT measured clearance. Poster presented at the 2017 Global Specialty Lens Symposium, Las Vegas. 2017 Jan.
10. Yeung D, Murphy PJ, Sorbara L. Objective and Subjective Evaluation of Clinical Performance of Scleral Lens with Varying Limbal Clearance in Keratoconus. Optom Vis Sci. 2020 Sep;97:703-710.
11. Kumar P, Carrasquillo K, Chaudhary S, Basu S. A multi-parameter grading system for optimal fitting of scleral contact lenses. F1000Res. 2022 Jan;11:6.
12. McMonnies CW. A hypothesis that scleral contact lenses could elevate intraocular pressure. Clin Exp Optom. 2016 Nov;99:594-596.
13. Walker MK, Pardon LP, Redfern R, Patel N. IOP and Optic Nerve Head Morphology During Scleral Lens Wear. Optom Vis Sci. 2020 Sep;97:661-668.
14. Chiu G. Rising Above the Surface. Contact Lens Spectrum. 2023 Jul;38:22-29.
15. Lam CSY, Tang WC, Tse D Y-Y, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomized clinical trial. Br J Ophthalmol. 2020 Mar;104:363-368.
16. Bao J, Yang A, Huang Y, Li X. One-year myopia control efficacy of spectacle lenses with aspherical lenslets. Br J Ophthalmol. 2021 Aug;106:1171-1176.
17. Rappon J, Neitz J, Neitz M, Chung C, Chalberg TW. Two-Year Effectiveness of a Novel Myopia Management Spectacle Lens with Full-Time Wearers. Invest Ophthalmol Vis Sci. 2022 Jun;63:408.
18. Liu X, Wang P, Xie Z, et al. One-year myopia control efficacy of cylindrical annular refractive element spectacle lenses. Acta Ophthalmol. 2023 Sep;101:651-657.
19. Huang Z, Chen XF, He T, Tang Y, Du CX. Synergistic effects of defocus-incorporated multiple segments and atropine in slowing the progression of myopia. Sci Rep. 2022 Dec;12:22311.
GSLS Awards


Poster Winners
This year’s Poster Session featured more than 140 posters on a wide variety of contact lens and other eyecare topics. The following were chosen as the best in their categories:

Research
First Place:
• Assessing Efficacy of a Dual-Focus Myopia Control Contact Lens for Faster and Slower Progressing Eyes by David Hammond (pictured above); Arthur Bradley; Baskar Arumugam; Martin Rickert; and Paul Chamberlain
Second Place:
• Two-year Myopia Management Efficacy of an Extended Depth of Focus Soft Contact Lens by Sergio Díaz-Gómez; Mercedes Burgos-Martínez; Padmaja Sankaridurg; Amaia Urkia-Solorzano; and Jesús Carballo-Álvarez
Third Place:
• Does Pupil Size Influence Vision Performance of a New Silicone Hydrogel Daily Disposable Multifocal Contact Lens (Kalifilcon A)? by Nitasha Phatak, MD, PhD; William Reindel, OS, MS; and Marjorie Rah, OD, PhD

Clinical Case Report/Series (Optometry Resident first author)
First Place:
• Corneal GP Lenses for Management of Irregular Astigmatism Secondary to Ocular Chemical Burn by Emmy Tian, OD (pictured above), and Dawn Lam, MSc, OD
Second Place:
• The Multistep Management Approach of a Pediatric Neurotrophic Keratitis Patient by Janna Pham, OD; Anna-Kaye Logan, OD; and Maria Walker, OD, PhD
Third Place:
• Resolution of Persistent Rebound Hyperemia After Scleral Lens Removal with Haptic Fenestrations by Yung Fen Chen

Clinical Case Report/Series (Non-Optometric Resident first author)
First Place:
• A Cautionary Tale: Visual Rehabilitation with Scleral Lens in a Case of Post-LASIK Ectasia with Form Fruste Keratoconus in the Fellow Eye by Sharon Qui, OD, MS (pictured above); and Chelsea Bray, OD
Second Place:
• Enhancing Vision Through Innovation: Profilometry-Based Scleral Lens Design for Advanced Post-Surgical Glaucoma Patient by Stephanie Pisano, OD
Third Place:
• Implementation of Vented Channels to Prolong Wear Time for a Patient with Scleral Lens-Induced Corneal Graft Edema by Chirag Patel, OD
Photo Contest Winners

Almost 50 photos were submitted for the annual GSLS Photo Contest. The winning photos appeared on the cover of the April 2024 issue of Contact Lens Spectrum. The winners (pictured left to right) are:
First Place: "Charlotte’s Web, Scleral Lens Edition" by Karen Carrasquillo, OD, PhD
Second Place: "Psychedelic Tear" by Vicente Berbegal Garcia