




AMNIOTIC MEMBRANE contact lenses play an active role in the management of ocular surface disease and corneal anomalies. They can act as bandages and deliver protection over the compromised corneas, provide a therapeutic solution, or offer cosmetic opportunities. They can be used to enhance corneal wound healing, improve corneal tissue hydration, reduce pain, and offer visual restoration by potentially reducing the risk of scar formation.
Amnio-grafts are used to accelerate healing of damaged ocular surface. Amniotic membranes are a therapeutic biological tissue that promotes epithelial surface reconstruction for wound healing. One of the most common indications for amniotic membrane is for chronic epithelial defects, especially if recurrent. By forming a scaffold and improving the spread of tear fluid over the ocular surface, epithelialization is promoted. The utilization of amniotic membrane is a successful tool for practitioners to employ on patients who are poor healers.1
An amniotic membrane has become a promoter for nonhealing epithelial defects to rebuild from various insults. Ocular surface disease, filamentary keratitis, limbal stem cell deficiency (LSCD), corneal erosions, infectious and inflammatory corneal ulcers, corneal bullous, chemical burns, epithelial basement membrane dystrophy, Stevens-Johnson syndrome, and neurotrophic keratitis can be protected by the same mechanism as a baby is protected by promoting new tissue growth, reducing pain and scar formation from the amniotic membrane.2 One of the advantages of using amniotic membrane therapy is there is no concern for rejection as they are avascular.3
The amniotic membrane consists of three layers,including a single layer of epithelial cells, a thick basement membrane, and an avascular stromal layer. These three layers improve the quality of wound healing, reduce scar formation, reduce pain, and allow for faster re-epithelialization.1
The usage of amniotic graft for the treatment of chronic/acute neuropathic wounds and ocular surface injuries has become safe, effective, and prevalent as evidenced by the numerous case histories found in the literature. The U.S. Food and Drug Administration (FDA) designation for clinical use of “allogeneic dehydrated and decellularized amniotic membrane is considered a 361 [human cells, tissues, and cellular and tissue-based products] HCT/P if the product is restricted to homologous use for a wound covering.”4
The basic function of the amniotic membrane is to protect the fetus from the surrounding environment. When the amniotic membrane is used for wound healing for its anti-scarring, antigenic, and anti-inflammatory ability, the therapy is no longer homologous. Promoting amniotic membrane applied to the surface of the eye as a covering and offering protection from the surrounding environment in ocular repair and reconstruction procedures is then homologous because of its basic functions is like amniotic membrane in utero.
The 361 HCT/P designation identifies that an amniotic membrane meets certain public safety measures without additional regulations because of its low risk of disease transmission. These regulations explain the types of HCT/Ps that do not require premarket approval; and the registration, manufacturing, and reporting steps that must be taken to prevent the introduction, transmission, and spread of communicable diseases by these HCT/Ps.5
The amniotic graft is not homologous when the graft is used with the epithelial side up with cytokines and extracellular fluid to promote anti‑scarring and anti‑inflammatory effects in wound recovery. It is homologous when the amniotic membrane product is used as a patch with the epithelial side down so that the biological bandage is protecting the tissue during repair and recovery.6
The ability to cover a wound with a biological bandage is both soothing and protective. Exposed nerve endings are calmed and fluid and heat losses are slowed, optimizing moisture balance. The underlying tissue is protected from shearing trauma from the eyeblink, inflammatory and autolytic responses modulated, and cellular interactions promoted to improve the overall healing process. Once considered medical waste, the unique regenerative properties of amniotic membranes allowed them to become a popular natural treatment agent for a variety of medical conditions.1
There have been renewed efforts to preserve placental tissue that retain their natural biological activities so the material can be safely and conveniently used as an allograft in a variety of clinical settings. There are many methods for processing human tissue, resulting in complete removal of cells and DNA, soluble macromolecules, and antigenic and immunogenic macromolecules, leaving only an extracellular scaffold.
Recently, a gentle cleansing and dehydration process was developed to preserve and maintain the biological activities inherent in the native amniotic membranes, retaining the natural growth factors and regulatory molecules naturally found in these placental tissues.7,8 This process has resulted in commercially available dehydrated human amnion/chorion membrane.
Types of amniotic membranes include cryopreserved amniotic membrane and dehydrated amniotic membrane. The hyaluronic acid that is retained in the cryopreservation process inhibits pro-inflammatory cells, suppresses T-cell activation, controls matrix metalloproteinases (MMP) production, and prevents scar formation. The overall extracellular matrix is responsible for cryopreserved amniotic membrane’s anti-inflammatory and healing properties, such as tissue repair and remodeling.6-8
The primary goal of cryopreserved and dehydrated amniotic membranes is to promote regenerative wound healing. Both products are homologous because of its protective indication during wound recovery. Cryopreserved amniotic membrane have been cleared by the FDA as a class II medical device, with product claims designated by the FDA including protective wound healing and anti-inflammatory effects. FDA-approved claims for dehydrated amniotic membrane are limited to wound coverage.9
There is concern about whether the dehydrated amniotic membrane retains its extracellular matrix of growth factors, including hyaluronic acid and heavy side-chain protein that provide anti-inflammatory and anti-scarring properties during wound recovery. The debate is whether the dehydrated form doesn’t retain the same anti-inflammatory effect during wound recovery. Additional scientific evidence is needed to either support or dispute.
Advantages/disadvantages of using dehydrated amniotic membrane from the authors’ clinical experience include comfort and no refrigeration, enabling easier storage compared to the cryopreserved counterpart.9
Further research and cross comparison between cryopreserved versus dehydrated is required. Limited studies show that cryopreservation retains the native architecture of the amniotic membrane/umbilical cord extracellular matrix and maintains the quantity and activity of key biological signals present in fresh amniotic membrane/umbilical cord, including high molecular weight hyaluronic acid, heavy chain-HA complex, and pentraxin.8 The dehydrated tissues were found to be structurally compromised and almost completely lacked these crucial components;10 however, they have been found to be clinically highly effective.11
The freeze-dried or dehydrated form doesn’t require any specialized refrigeration, can be kept on the shelf, and used when needed. In essence, the clinician just hydrates it as needed.9
The concern with this form is whether it actually retains all the hyaluronic acid with a heavy side-chain protein that provides the anti-inflammatory effect. Overall, it appears that the dehydrated form doesn’t retain as much anti-inflammatory effect. There are two primary contraindications for amniotic membranes: Patients who have glaucoma drainage devices or filtering blebs and—for one particular membrane—include patient’s allergies to ciprofloxacin or amphotericin B.12
Ocular surface disease encompasses multiple etiologies and disorders of diverse pathogenesis. It may be defined as “any disorder affecting the integrated functional structures of the ocular surface…”13 Ocular surface disease accounts for a frequent cause of visits to eyecare practitioners annually.14
Inflammation is the first sign of wound healing and also the hallmark of all ocular surface disease. Uncontrolled inflammation leads to chronic pain and discomfort/irritation, delayed healing, more tissue damage, and vision-threatening complications (scar/haze). Effective control of inflammation is an important strategy to promote speed and quality of healing, faster re-epithelization, and active intervention against scar formation, consequently improving the rate of corneal clarity.15
The corneal epithelium acts as a protective barrier to infectious agents and maintains a smooth optical surface.15 An insult to the epithelium results in a defect (corneal erosion) that predisposes the cornea to infection and reduces quality of vision. In normal conditions, the defect is healed when the epithelial layer undergoes an active repair process involving regulated growth factors, cellular signaling, proliferation, migration, and extracellular matrix remodeling.15
Katzman reported that persistent corneal epithelial defects (PEDs) result from the failure of re-epithelialization and closure within 10-14 days after a corneal injury despite standard treatment.16 Potential etiologies include defective epithelial adhesion, LSCD, inflammation, neurotrophic components, and idiopathic/hereditary disorders.16Management involves a stepwise approach depending on etiology.
Nonsurgical modalities include optimization of the ocular surface, bandage contact lenses (BCLs), blood derived products (e.g., autologous serum and platelet-rich plasma eye drops), punctal plugs, and scleral contact lenses.17Subsequent surgical treatment options include epithelial debridement, amniotic membrane transplant (AMT), and corneal stem cell transplant.18
The primary etiology of the PED was LSCD (n = 5/9) due to Stevens-Johnson syndrome (n = 2/5), glaucoma procedures (n = 1/5), graft-versus-host disease (n = 1/5), and severe allergic reaction (n = 1/5). Additional etiologies included neurotrophic cornea post keratoplasty (n = 2/9) and severe dry eye disease (n = 2/9).16
Amniotic membranes have been proven to be effective treatment of PEDs as a result of their plethora of growth factors that help facilitate anti-inflammatory properties.18
CASE REPORT: PERSISTENT EPITHELIAL DEFECT
A 43-year-old female presented with pain, photophobia, and discharge for the past few months.
• Patient ocular history: dry eyes for the past 10 years, managed with over-the-counter artificial tears.
• Diagnosis: superficial punctate keratitis with epithelial defect (Figure 1).
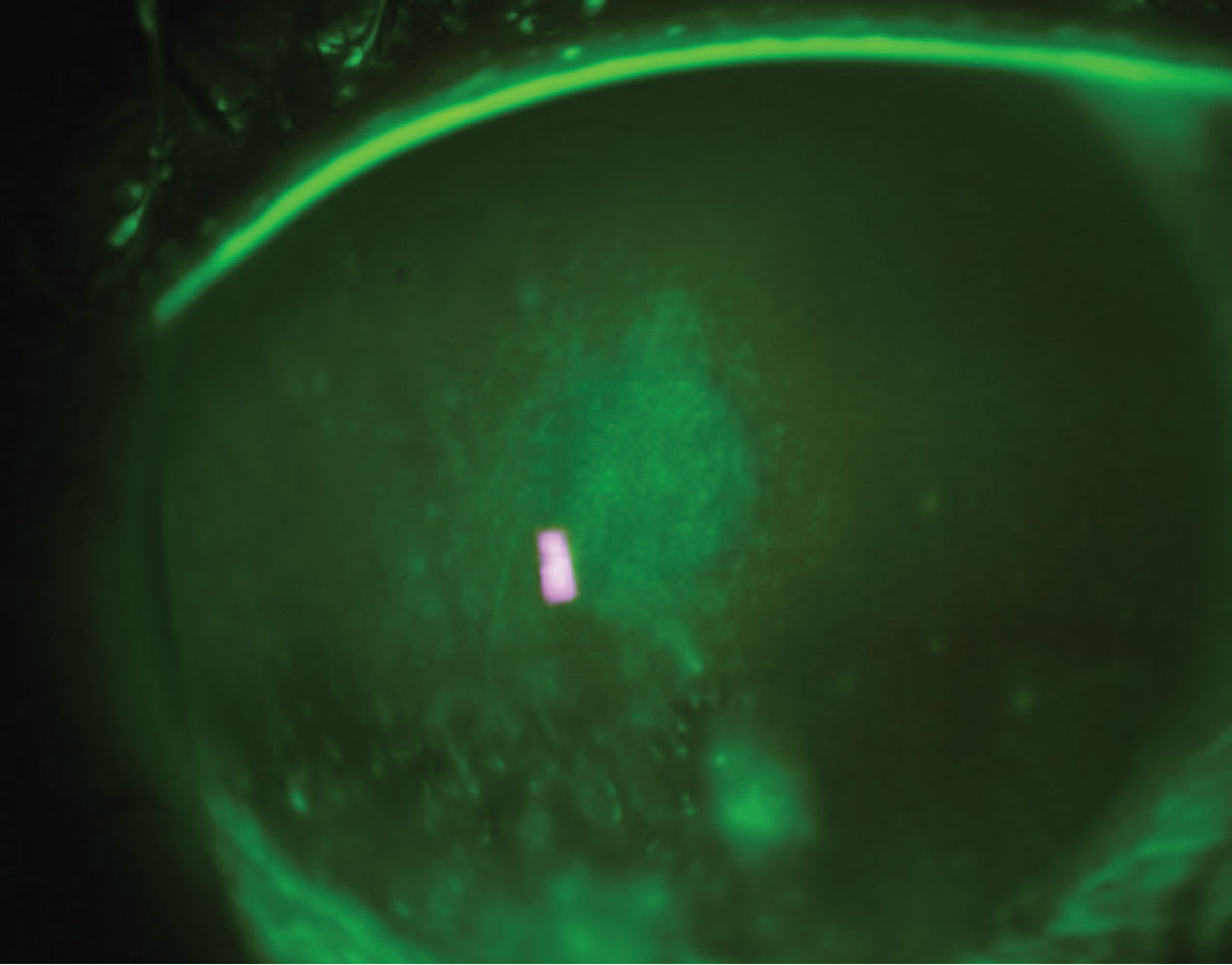
• Treatment: dehydrated amniotic membrane contact lens (AMCL) 12mm biostability amnio graft was inserted in the bowl of soft contact lens, 8.4mm base curve radius (BCR); 14.0mm overall diameter (OAD); –0.50D.
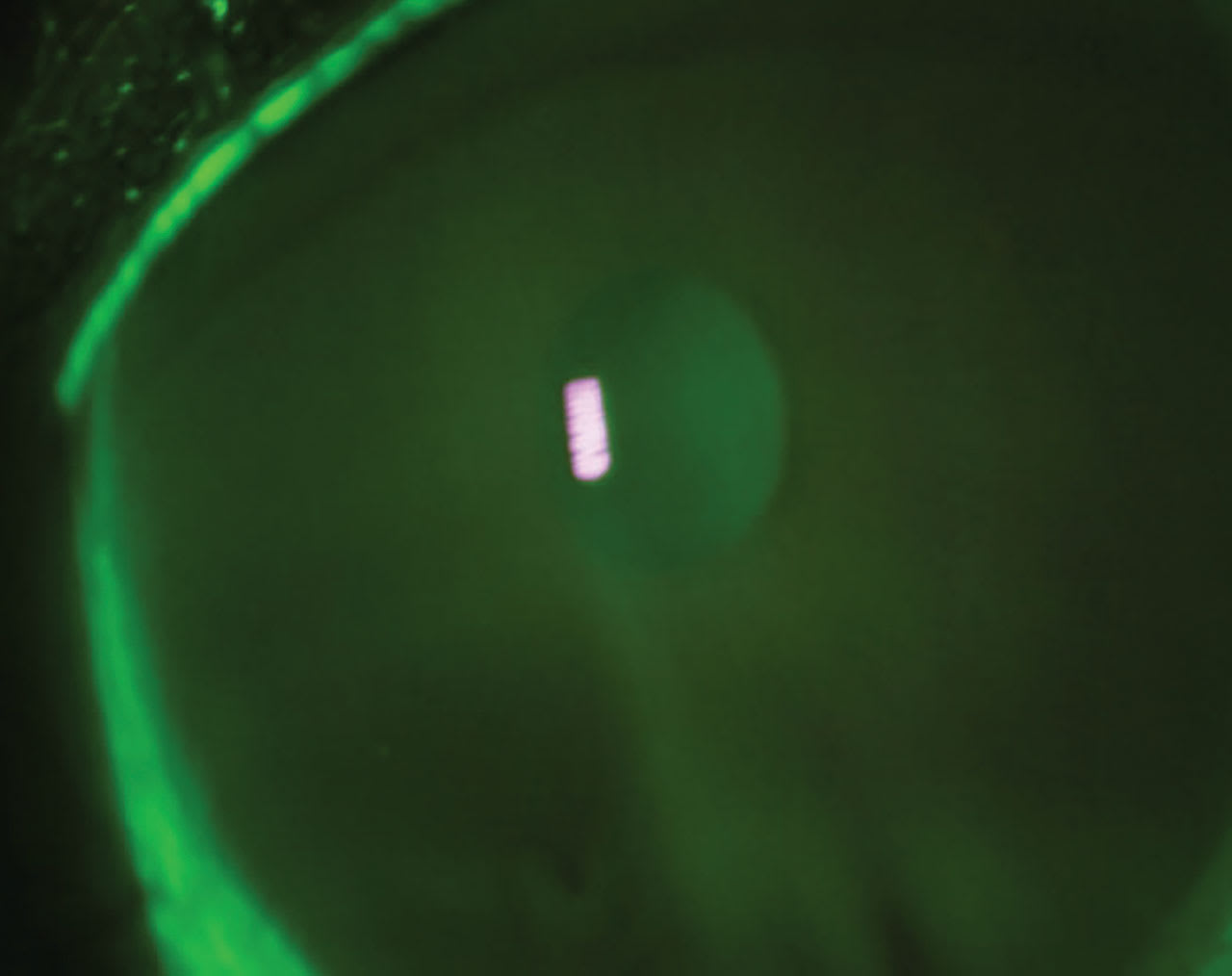
• Follow-up at 48 hours demonstrated a clear cornea (Figure 2).
CASE MANAGEMENT FOR ANTERIOR SEGMENT PATHOLOGY: USING CRYOPRESERVED AMCL
A 44-year-old male presented to the clinic with a chief complaint of severe pain, along with photophobia in his right eye for the past few days.
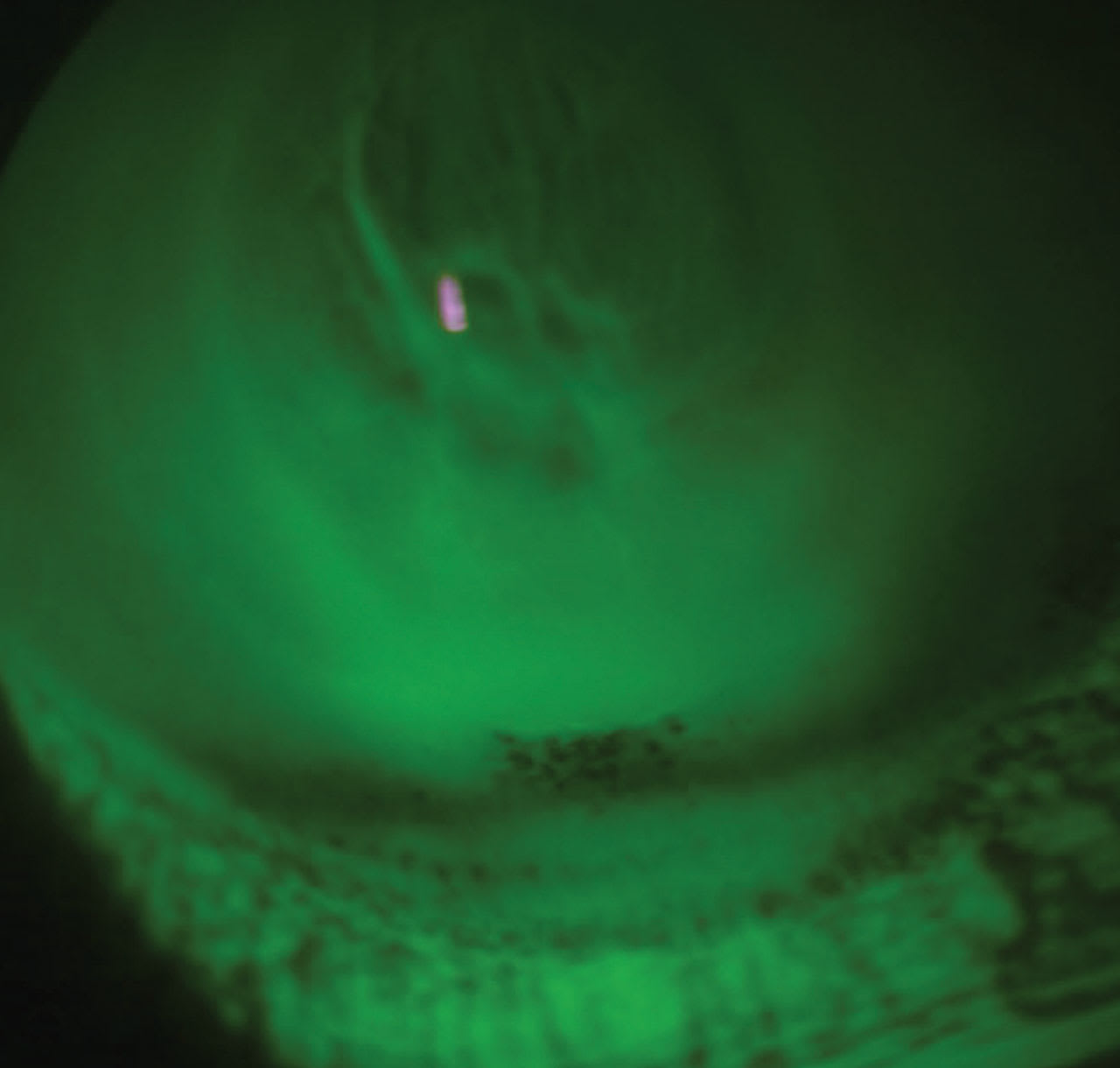
• Patient ocular history: ectasia secondary to laser-assisted in situ keratomileusis (LASIK) surgery for the past few years. The patient admitted to sleeping in his scleral contact lenses. Figure 3 displays the anterior segment image.
• Diagnosis:
1) corneal ulcer
2) ectasia
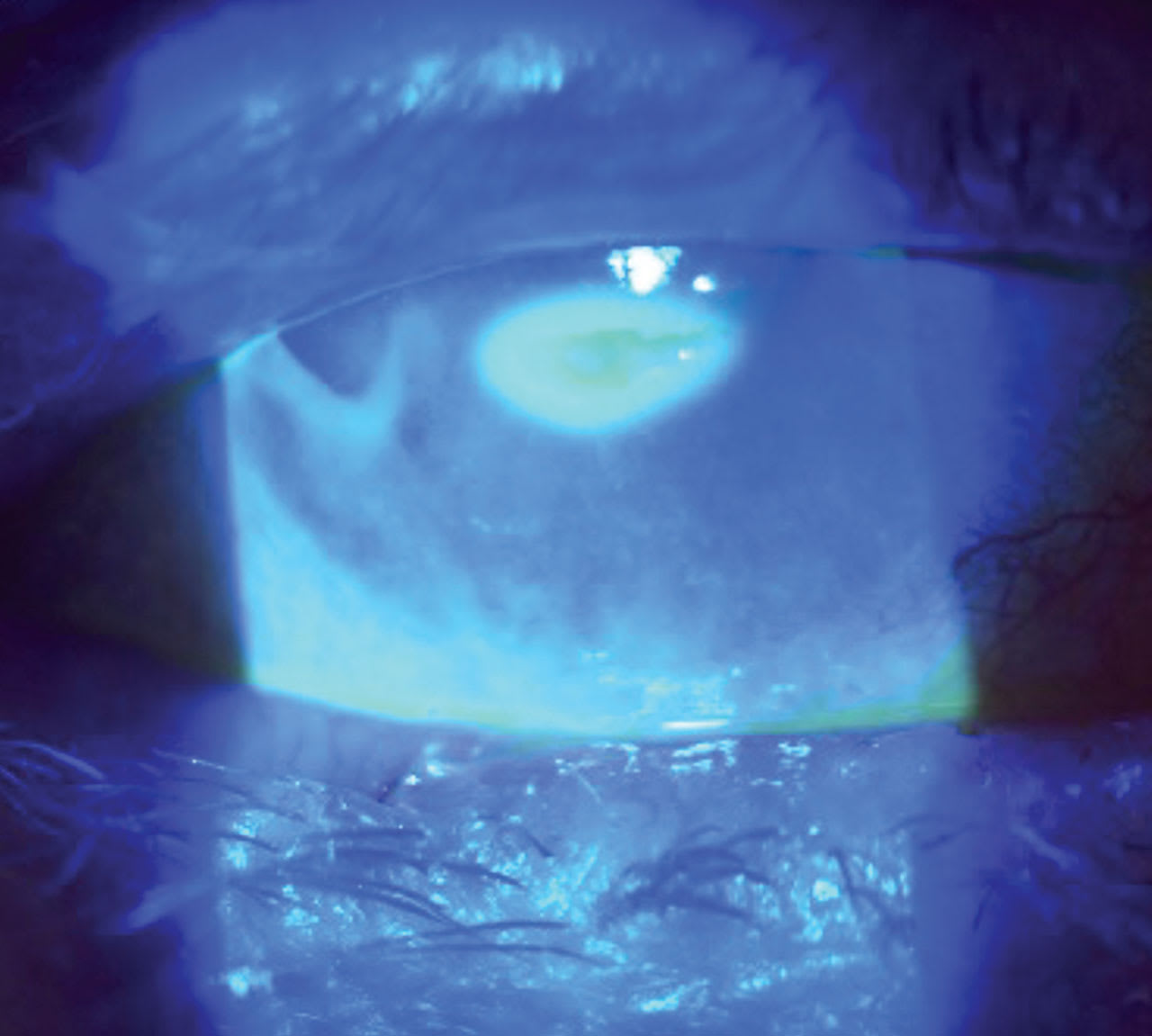
• Treatment: Approaching a compromised cornea with underlining conditions such as keratoconus or post-refractive complications must be aggressive but guarded. In this case, it was a cryopreservative slim-profile amniotic membrane, besifloxacin q.i.d. to the affected eye, and artificial tears every 30 minutes. Figure 4 shows the eye with an AMCL over the compromised cornea. Figure 5 shows an image three days after removal.
Impairment to the trigeminal nerve adversely affects both blinking and tearing leading to severe ocular surface disease. The partial or total damage to the trigeminal nerve leads to inflammation, epithelial defects, stromal ulcerations, and deficiency of epithelial repair.19 Herpes zoster,20 trigeminal neuralgia,21 herpes simplex,22 and neurotrophic keratitis can initiate the sequence of events that lead to loss of corneal nerve density resulting in loss of vision, loss of corneal sensitivity, and scar formation. An early sign of corneal nerve damage is corneal staining with the loss of corneal sensitivity.19 Using this diagnostic marker can help identify the disease process.
Mackie classification separated neurotrophic keratitis (NK) into three stages.23 Clinical presentation of NK ranges from subtle corneal surface irregularities to corneal melting and perforation.19
The first stage is characterized by epithelial punctate keratitis, epithelial hyperplasia, stromal scarring, and corneal neovascularization. The second stage is defined by recurrent or persistent epithelial defects in the paracentral area with opaque epithelium. Descemet’s folds and anterior chamber inflammation may be observed.
This stage can mimic recurrent cornea erosion characterized with reduced lubrication and abnormal corneal epithelium with an absence of ocular discomfort. The third stage is characterized by stromal involvement with stromal corneal ulcer and infiltrate, which may result in corneal perforation and/or corneal thinning.23
The treatment is to protect the corneal epithelium and prevent an epithelial breakdown to reduce scar formation.24Amniotic membrane provides the necessary biological properties to offer a therapeutic remedy for a positive outcome. The epithelium of the amniotic membrane provides growth factors and cytokines useful for limbal stem cell.25
The basement membrane provides collagen and fibronectin to improve epithelial cell migration and adhesion to basal cells. This layer serves as a scaffold for limbal epithelial stem cells.2 The stromal matrix provides transforming growth factors, anti-inflammatory and blood vessel growth inhibition suppressing fibroblast proliferation and neovascularization.
The goal is to support epithelial adhesion and growth, as well as prolong the health of the cornea.26 The need for additional studies will provide scientific evidence to promote increased corneal nerve density regeneration by cryopreserved amniotic membrane.27
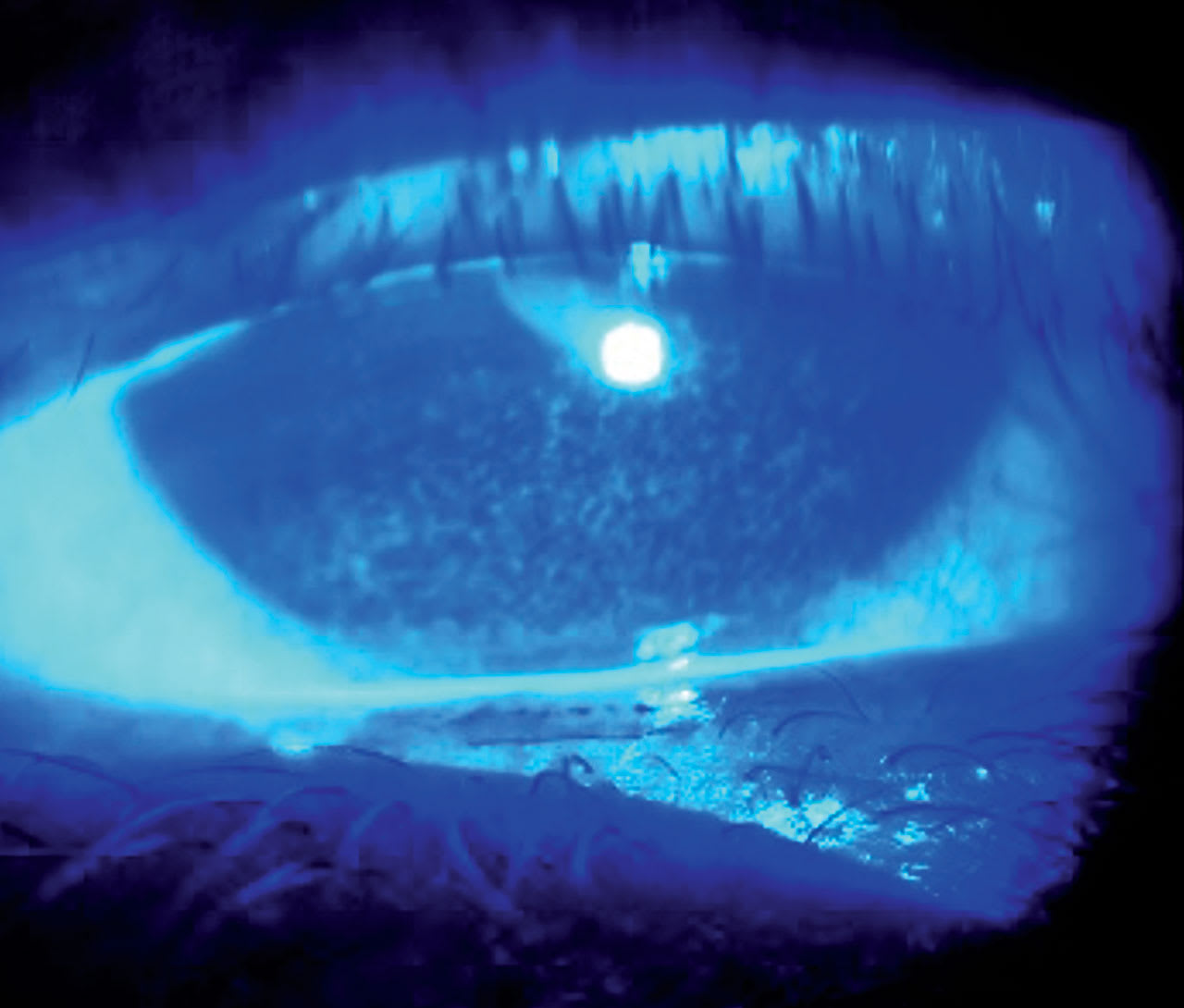
CASE REPORT: NEUROTROPHIC CORNEAL ULCER
An 81-year-old female presented with blurry vision, hyperemia, and a feeling of soreness. Slit lamp examination demonstrated a perforated neurotrophic corneal ulcer with subjective decreased corneal sensitivity, burning, and normal lacrimation (Figure 6). She had a history of Frey’s syndrome, rheumatoid arthritis, and Sjögren’s.
A cryopreserved amniotic membrane was placed on her eyes for two days. The amniotic membrane had completely dissolved when removed. The patient was instructed to use omega-3s 1000mg and vitamin A ointment at night.
Filamentary keratitis is another derivative of ocular surface disease defined by the presence of filaments on the surface of the cornea.28 The risk of filamentary keratitis increases with alterations of the tear film induced by friction with deficient aqueous tears. These filaments consist of mucin and epithelial cells.
Symptoms include pain and photophobia from epithelial non-healing defects and blurred vision from the surface disruption and the attachment of filaments onto the cornea. Epithelial corneal defects provide a site for these mucoid filaments to anchor. Patients often complain of symptoms such as persistent foreign body sensation, redness, and sensitivity to light, which may vary from moderate to severe in intensity.28
During reduced tear production, increased tear osmolarity creates excessive mucous strands and debris that adhere to the defective corneal epithelium and basement membrane. The aqueous deficient tear layer results in friction between the eyelid and ocular surface, which increases the production of mucus by the conjunctival goblet cells.28 During the blink, the upper lid tugs on these filaments, resulting in pain, inflammation, and increased epithelial defects.28
Filamentary keratitis develops from inflammatory cells and fibroblasts present just below the basal epithelium disrupting the epithelial basement membrane and Bowman’s layer.28 Additionally, friction from blinking and eye movement with injured epithelium and a deficient tear film produces the filaments. Further shear pressure by the eyelid, mucin, conjunctival epithelium, and inflammatory cells results in building up the filament. This phenomenon is associated with inflammation and the detachment of basal cells from the Bowman’s layer due to blinking and eye-movement-related mechanical friction.29
Treatments include dissolving the filaments with a mucolytic agent acetylcysteine, non-preserved lubrication, punctal occlusion, anti-inflammatories, a bandage contact lens, and amniotic membrane.30
Therapy is focused on increasing the aqueous component of the tears through punctal occlusion and non-preserved tear drops. Amniotic membrane, with its anti-inflammatory and wound healing properties, results in reduction of scar formation and re-epithelization accelerating the recovery time. The amniotic membrane also actively acts as a shield between the cornea and upper lid for a faster recovery.31
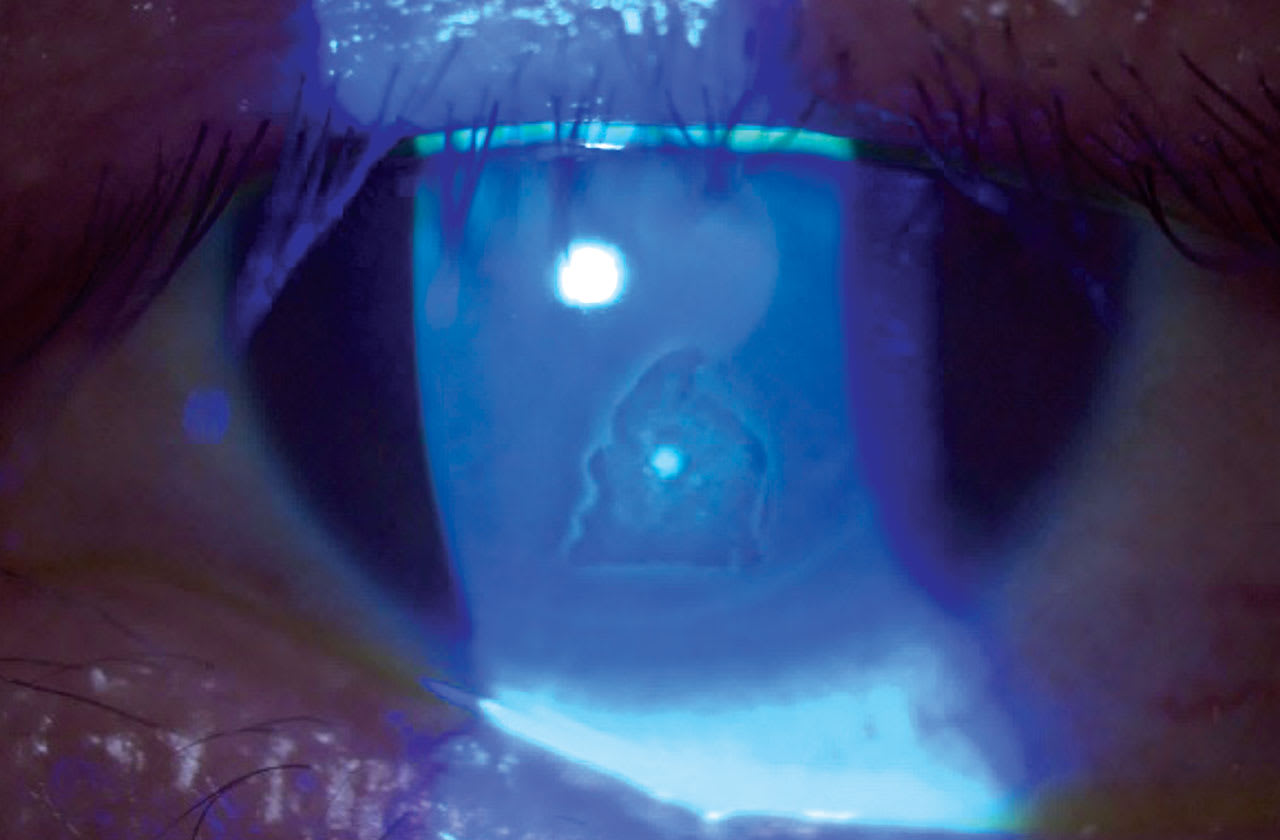
CASE REPORT: RHEUMATOID ARTHRITIS
A 50-year-old female presented with symptoms of blurry vision photophobia, foreign body sensation, and tearing for the previous two weeks. The patient had a history of rheumatoid arthritis and dry mouth. The visual acuity was 20/30-2OS. Anterior segment examination revealed superficial punctate keratitis 2++ that was diffuse throughout the cornea (Figure 7). The diagnosis was filamentary keratitis.
A dehydrated amniotic membrane was placed on the eye for three days and she was prescribed loteprednol ophthalmic suspension q.i.d. At the follow-up visit three days later, the membrane was removed and the patient reported no pain with the return of normal vision. Treatment continued with oil-based artificial tear eye drops, vitamin A ointment before bedtime, and oral omega-3 therapy.
Typical clinical signs and symptoms of recurrent corneal erosion are eye pain, redness, photophobia, blurred vision, and tearing upon awakening in the morning. These symptoms are caused by the epithelial defect and will last until the surface disruption has healed. These episodes are often noninfectious and corneal anesthesia is normal. Recurrent corneal erosion is characterized by inadequate epithelial basement membrane adhesions, resulting in repeat episodes of corneal epithelial defects.32
Adhesions between the palpebral conjunctiva of the eyelids and the corneal epithelium in patients who have punctate epitheliopathy contribute significantly to recurrent corneal erosions. Individuals who have ocular rosacea are particularly at risk due to meibomian gland dysfunction and resultant evaporative dry eye disease.
Recurrent corneal erosion usually develops three to 10 days after a corneal injury, although it can develop several months later. After the insult to the corneal surface, inflammation ensues, causing the disruption in the extracellular adhesion of the epithelium. MMP have been implicated in the degrading of the cellular construction.32
This results in poor adhesion of the corneal epithelium to Bowman’s membrane due to accumulation of inflammatory components interfering with the anchoring mechanism.32 The anchoring mechanism that provides attachment between the basement membrane, Bowman’s layer, and stroma are the hemidesmosomes located in the corneal basal epithelial cells.32 Corneal erosions are formed when these hemidesmosomes no longer adhere the epithelial cells to the basement membrane.32 The anti-inflammatory and anti-scarring properties of amniotic membranes inhibit MMPs rendering them as a therapy for recurrent corneal erosion.33
CASE REPORT: ULCERATIVE COLITIS
A 37-year-old female with a history of ulcerative colitis presented with foreign body sensation, tearing, and sensitivity to light for the past few days. The cornea had positive epithelial diffused horizontal fluorescein staining in the inferior third (Figure 8). The patient worked in a grocery store stocking products in the freezer. Due to her environment and the amount of time in the cooler with reduced humidity, the patient reported that symptoms appeared more frequently on days at work.

Upon ocular examination, large lacrimal punctum were observed along with incomplete blinking. A dehydrated membrane was placed on her eye and occluded the inferior punctum. The follow-up evaluation was scheduled for two days, in which the AMCL was removed and consequently the insult was completely resolved. The patient was educated about proper blinking, prescribed blinking exercises, and the patient’s husband was requested to observe whether the lids were closed during sleep.
During recovery, vitamin A therapy has been shown to help heal the defective epithelium. Corneal epithelial cells produce hyaluronic acid promoting epithelial wound healing properties for adhesion and tissue migration. Retinyl palmitate also stimulates the production of hyaluronic acid34 and mucin,35 aiding in repairing corneal epithelial cell damage.
Retinyl palmitate (vitamin A) ophthalmic therapy will help stabilize the mucin layer, which is one of the causes of corneal and conjunctival epithelial wound recovery from epithelial defects.33 After the application of amniotic membrane, retinyl palmitate can help in the wound healing process.36
CASE REPORT: RECURRENT CORNEAL EROSION
A 50-year-old male presented in the office with an ocular history of recurrent painful red eye along with sensitivity to light. The patient woke up in the morning without history of incident. This presentation had occurred at least five times over the last three years. The patient was diagnosed with recurrent corneal erosion (Figure 9).
For treatment, a cryopreserved amniotic membrane was placed on the eye for three days. The amniotic membrane was removed, and the cornea was completely epithelialized without any fluorescein staining. Therapy at night before bedtime included heat and vitamin A ointment. The patient has been without incident for the past 18 months.
SUMMARY
The use of amniotic membrane in patients who have non-healing epithelial defects improves patient comfort, vision, and resolves some of the corneal anomalies that affect the patient’s quality of life. The application of these biological bandages can offer a positive therapeutic effect on any inflammatory, mechanical, viral, and bacterial disease process disrupting the corneal tissue.
The anti-inflammatory, antiangiogenic, anti-scarring, and antimicrobial properties reduce the risk of corneal scar formation, epithelial proliferation, and nerve regeneration. The future of using amnio-grafts’ biological properties lies in the development of multiple applications that can be applied directly to the eye.37,38
REFERENCES
1. Dadkhah Tehrani F, Firouzeh A, Shabani I, Shabani A. A Review on Modifications of Amniotic Membrane for Biomedical Applications. Front Bioeng Biotechnol. 2021 Jan 13;8:606982.
2. Tighe S, Mead OG, Lee A, Tseng SCG. Basic science review of birth tissue uses in ophthalmology. Taiwan J Ophthalmol. 2020 Mar 4;10:3-12.
3. Miller R. Amniotic Membranes to the Rescue. Modern Optometry. 2021 April:52-54.
4. U.S. Food and Drug Administration. Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation and Homologous Use. Center for Biologics Evaluation and Research, Center for Devices and Radiological Health. 2020 July. Available at fda.gov/regulatory-information/search-fda-guidance-documents/regulatory-considerations-human-cells-tissues-and-cellular-and-tissue-based-products-minimal. Accessed 2024 Feb 19.
5. Schechter BA. Amniotic Membrane Transplant (letter to the editor: author’s reply). Cornea. 2006 April;25:368-369.
6. Dallal MMS, Nikkhahi F, Imeni SM, et al. Amniotic Membrane Transplantation for Persistent Epithelial Defects and Ulceration due to Pseudomonas Keratitis in a Rabbit Model. J Ophthalmic Vis Res. 2021 Oct 25;16:552-557.
7. U.S. Patent and Trademark Office. MiMedx U.S. Patents: PURION® Process U.S. Patent 8,357,403-Placenta Tissue Grafts. U.S. Patent 8,372,437-Placenta Tissue Grafts. U.S. Patent 8,409,626-Placenta Tissue Grafts. Available at uspto.gov/patents/search. Accessed 2024 Feb 26.
8. Koob TJ, Rennert R, Zabek N, et al. Biological properties of dehydrated human amnion/chorion composite graft: implications for chronic wound healing. Int Wound J. 2013 Oct;10:493-500.
9. Mcgaughy AG, Gupta PK. In-office use of amniotic membrane. EyeNet. 2015 Feb;31-32.
10. Chua L, Cooke M, Mandrycky, et al. Biological differences between cryopreserved and dehydrated amniotic membrane tissue grafts. Invest Ophthalmol Vis Sci. 2013 Jun;54:3894.
11. Allen CL, Clare G, Stewart EA, et al. Augmented Dried versus Cryopreserved Amniotic Membrane as an Ocular Surface Dressing. PLoS One. 2013 Oct;8:e78441.
12. Prasher P, Lehmann JD, Aggarwal NK. Ahmed tube exposure secondary to prokera implantation. Eye Contact Lens. 2008 Jul;34:244-245.
13. Pensyl CD. Preparations for dry eye and ocular surface disease. In: Bartlett JD, Jaanus SD, eds. Clinical Ocular Pharmacology 5th ed. 2007:263-278.
14. Mehra D, Cohen NK, Galor A. Ocular surface pain: A narrative review. Ophthalmol Ther. 2020 Sep; 9:1-21.
15. Mobaraki M, Abbasi R, Omidian Vandchali S, Ghaffari M, Moztarzadeh F, Mozafari M. Corneal Repair and Regeneration: Current Concepts and Future Directions. Front Bioeng Biotechnol. 2019 Jun 11;7:135.
16. Katzman LR, Jeng BH. Management strategies for persistent epithelial defects of the cornea. Saudi J Ophthalmol. 2014 Jul;28:168-172.
17. Mimouni M, Trinh T, Sorkin N, et al. Sutureless dehydrated amniotic membrane for persistent epithelial defects. Eur J Ophthalmol. 2022 Apr 22;32:875-879.
18. Dhillon HK, Bahadur H, Raj A. A comparative study of tarsorrhaphy and amniotic membrane transplantation in the healing of persistent corneal epithelial defects. Indian J Ophthalmol. 2020 Jan;68:29-33.
19. Semeraro F, Forbice E, Romano V, et al. Neurotrophic keratitis. Ophthalmologica. 2014;231(4):191-197.
20. Cho YK, Kwon J, Pugazhendhi S, Ambati BK. Maxillary Zoster and Neurotrophic Keratitis following Trigeminal Block. Case Rep Ophthalmol. 2019 Feb 6;10:61-66.
21. Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014 Mar 19;8:571-579.
22. Cheng AMS, Tseng SCG. Self-Retained Amniotic Membrane Combined With Antiviral Therapy for Herpetic Epithelial Keratitis. Cornea. 2017 Nov;36:1383-1386.
23. Kordić R, Kuzman T, Popovic-Suic S, Kalauz M, Ćurković T. Neurotrophic Keratopathy: Case Report. Acta Clin Croat. 2007;46(Suppl 1):117-120.
24. Feroze KB, Patel BC. Neurotrophic Keratitis. StatPearls Publishing. 2023 Jan.
25. Yoon JJ, Ismail S, Sherwin T. Limbal stem cells: Central concepts of corneal epithelial homeostasis. World J Stem Cells. 2014 Sep 26;6:391-403.
26. Dadkhah Tehrani F, Firouzeh A, Shabani I, Shabani A. A Review on Modifications of Amniotic Membrane for Biomedical Applications. Front Bioeng Biotechnol. 2021 Jan 13;8:606982.
27. John T, Tighe S, Sheha H, et al. Corneal Nerve Regeneration after Self-Retained Cryopreserved Amniotic Membrane in Dry Eye Disease. J Ophthalmol. 2017;2017:6404918.
28. Lee SM, Jun RM, Choi KR, Han KE. Clinical manifestation and risk factors associated with remission in patients with filamentary keratitis. Am J Ophthalmol. 2020 Oct;218:78-83.
29. Hidetoshi T, Norihiko Y, Aoi K, et al. Investigation of the corneal filament in filamentary keratitis. Invest Ophthalmol Vis Sci. 2009 Aug;50:3696-3702.
30. Ditmars F, Brondeel K, Fagg W, Theriot P. A Double-Header: Dry Eye and Filamentary Keratitis. Modern Optometry. 2022 March.
31. Harthan J, Sicks L. Sutureless amniotic membranes (prokera) for filamentary keratitis: A case series.J Dry Eye Occ Surf Dis. 2019 May:e10-e16.
32. Miller DD, Hasan SA, Simmons NL, et al. Recurrent corneal erosion: a comprehensive review. Clin Ophthalmol. 2019 Feb;1113:325-335.
33. Vaidyanathan U, Hopping GC, Liu HY, et al. Persistent Corneal Epithelial Defects: A Review Article. Med Hypothesis Discov Innov Ophthalmol. 2019 Fall;8:163-176.
34. Toshida H, Tabuchi N, Koike D, et al. The effects of vitamin A compounds on hyaluronic acid released from cultured rabbit corneal epithelial cells and keratocytes. J Nutr Sci Vitaminol. 2012;58(4):223-229.
35. Kubo Y, Arimura A, Nakayasu K, Kanai A. Effect of vitamin A palmitate on the synthesis of mucins in cultured conjunctiva. Nippon Ganka Gakkai Zasshi. 1999 Aug;103(8):580-583.
36. Polcz ME, Barbul A. The Role of Vitamin A in Wound Healing. Nutr Clin Pract. 2019 Oct;34:695-700.
37. Mobaraki M, Abbasi R, Omidian Vandchali S, Ghaffari M, Moztarzadeh F, Mozafari M. Corneal Repair and Regeneration: Current Concepts and Future Directions. Front Bioeng Biotechnol. 2019 Jun 11;7:135.
38. Murri MS, Moshirfar M, Birdsong OC, Ronquillo YC, Ding Y, Hoopes PC. Amniotic membrane extract and eye drops: a review of literature and clinical application. Clin Ophthalmol. 2018 Jun 18;12:1105-1112.