



SPECIALTY LENS FITTERS often use glasses, soft lenses, or GP lenses to correct ametropia and astigmatism for patients who have keratoconus. It is the rigid nature of the GP material used to make corneal or scleral lenses that allows them to additionally correct for irregular astigmatism by masking the front-surface deformity of the keratoconic cornea using the tear layer or fluid reservoir (Hussoin et al, 2012).
Unfortunately, keratoconus patients can also have back-surface corneal irregularity leading to higher-order aberrations (HOAs) that are not corrected by GP lenses with standard front-surface optics. This is why many keratoconus patients still don’t achieve a 20/20 outcome despite having clear corneas. The case presented is a patient who had significantly improved visual acuity (VA) with the use of added front-surface asphericity.
A 42-year-old female keratoconus patient was referred for decreased VA with her newly fit scleral lenses. She had a history of corneal cross-linking a few years prior but no other surgeries or ocular disorders. The patient’s VA with her current scleral lenses was 20/60 OD and 20/50 OS.
Her right eye did improve to 20/40 with a +2.00D sphere over-refraction, but the measurement was variable. Slit lamp exam revealed well-fitting scleral lenses that exhibited adequate corneal clearance without compression or edge lift of the landing zone. Aberrometry measurements over the scleral lenses revealed clinically significant amounts of residual positive coma.
The patient was refit into a new pair of scleral lenses with updated powers using over-refractions (Figure 1). A proprietary amount of eccentricity to create a front surface aspheric change to the lenses significantly decreased the residual coma for both eyes (Figure 2). The patient’s visual acuities improved to 20/20 OD and 20/30 OS.
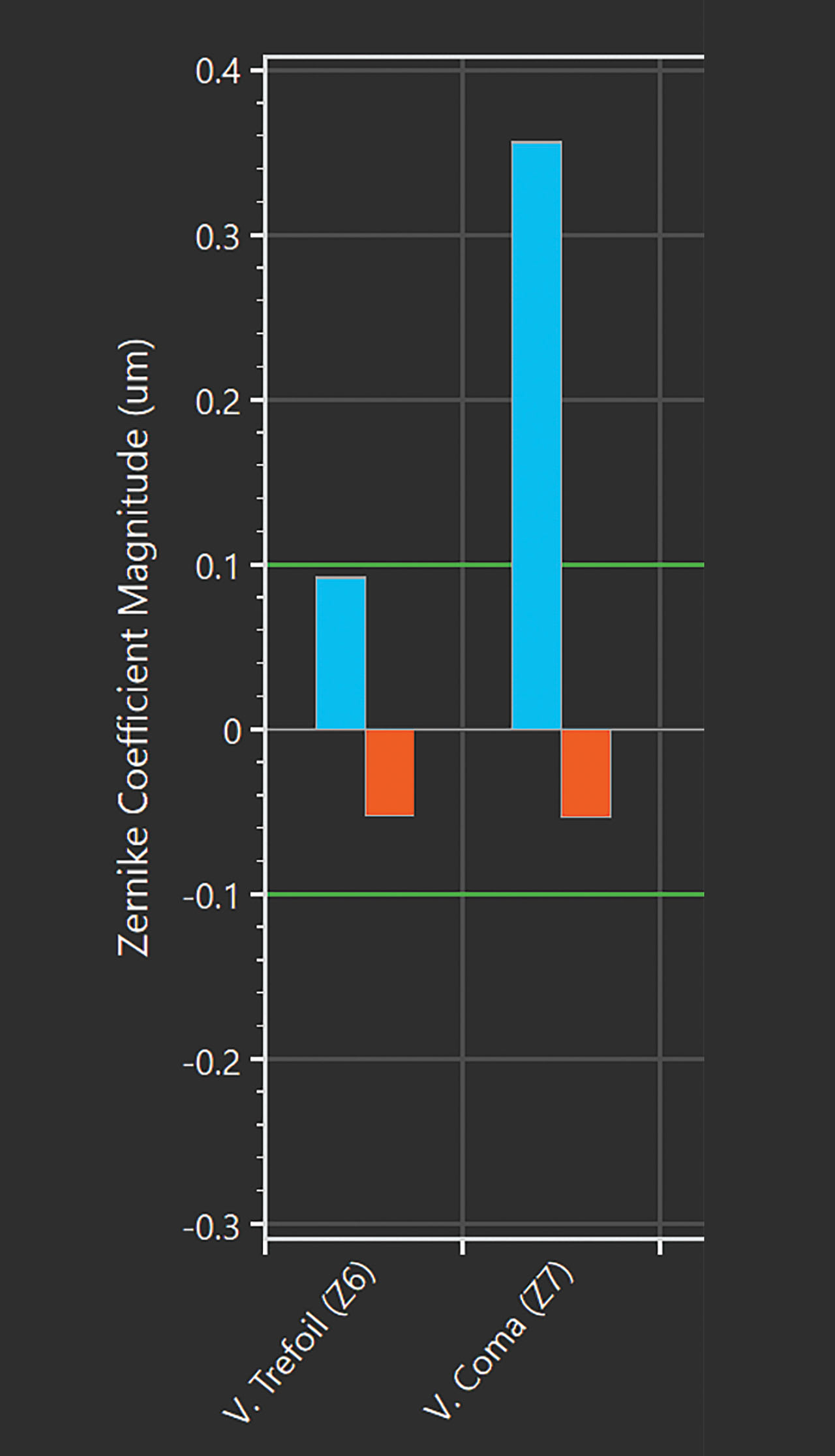
The residual coma she had while wearing her scleral lenses with standard optics was significant enough to decrease her visual acuity, and flipping the coma sign from negative without a lens to positive with a lens could also be disruptive because the patient was neuro-adapted to negative coma. Eccentric changes to the front surface to create asphericity tend to have the most impact by decreasing the amount of residual coma (Hussoin et al, 2012).
The literature suggests using eccentricity values that range from 0.3 to 0.8 to reduce residual coma (Badrinarayanan et al, 2023). Trialing different eccentric changes is currently the best way to know whether there are any objective or subjective improvements. A recent paper by Badrinarayanan and colleagues suggests that 0.6 is the most effective and commonly dispensed eccentricity value (Badrinarayanan et al, 2023).
Another approach to correct this patient’s residual HOA would be to use wavefront optics from aberrometry measurements to specifically correct each type of residual HOA. However, the advantages of using a uniform eccentric change that creates asphericity is that it can be added even if aberrometry measurements aren’t available, and the lenses don’t have to be rotationally stabilized for the optical correction to be effective.
REFERENCES
1. Hussoin T, Le HG, Carrasquillo KG, Johns L, Rosenthal P, Jacobs DS. The effect of optic asphericity on visual rehabilitation of corneal ectasia with a prosthetic device. Eye Contact Lens. 2012 Sep;38:300-305.
2. Badrinarayanan A, Balakrishnan AC, Dutta R, Kumar RM, Iqbal A. Impact of Scleral Lens Front Surface Eccentricity on Visual Acuity, Contrast Sensitivity, and Higher-Order Aberrations in Eyes With Keratoconus. Eye Contact Lens. 2023 Sep 1;49:374-378.