



CONTACT LENS follow-up appointments usually go one of two ways: the patient is happy, their vision is great, the ocular surface is healthy, and the lens fits well; or there is an unhappy patient who has blurred vision. In many cases, the patient and the practitioner are quick to blame the contact lens as the culprit, but it is important to remember how underlying ocular surface issues may reveal themselves and how the contact lens can impact these. The patient’s ocular surface, meibomian glands, lid margins, lashes, and periocular skin can reveal how successful their contact lens journey will be.
A 33-year-old female was fit into custom soft lenses due to high astigmatism. At the dispensing appointment, the fit was appropriate, vision was at the expected level, and her lens comfort was great. However, at the follow-up appointment after starting lens wear, she described significantly blurred 20/50 vision with transient moments of clarity. She also noted worsening discomfort with increased wear time and prolonged screen use.
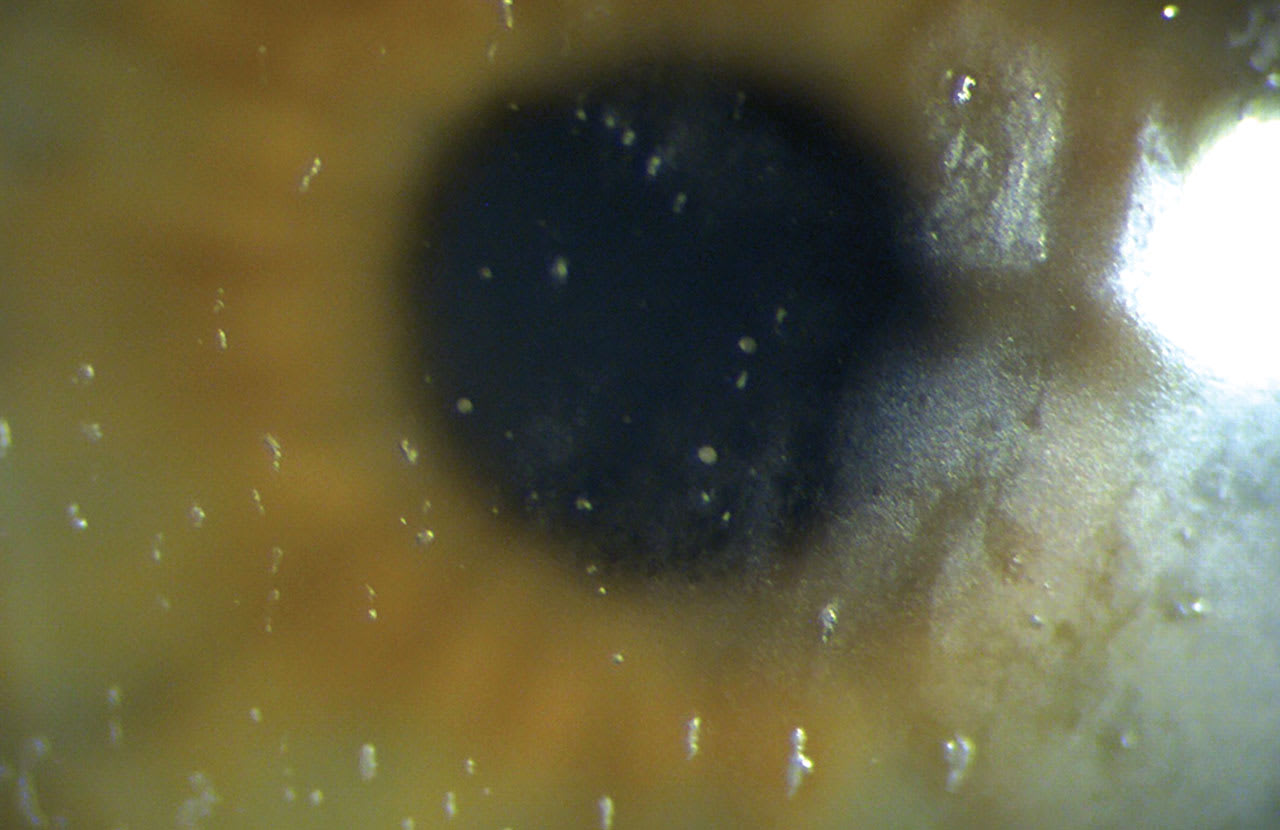
Upon evaluation of the lenses, the fit was deemed appropriate with adequate movement, coverage, and centration. The high amount of astigmatism in the lenses had adequate stability and minimal rotation. The lenses exhibited poor surface wettability and deposits that did not resolve with blinking (Figure 1).
The patient was over-refracted to assess whether additional power was needed in the lenses, and this revealed a high amount of additional cylinder power without a clear or good-quality endpoint. After removing the lenses, the patient’s ocular surface was assessed, revealing a significantly low tear breakup time, and poorly expressing meibomian glands, but no significant corneal staining.
When the patient was questioned further, she said she did not regularly remove her makeup or eyeliner. Instead, she removed it in the morning using an oil-based cleanser and then applied the contact lenses. Residual cleanser likely was adhering to the lens surface.
To improve a patient’s success with contact lenses, it is important to treat the underlying issues related to the ocular surface specific to the patient’s needs (Stapleton et al, 2021). Contact lens wear can also induce dry eye-related symptoms with or without the presence of typical dry eye clinical signs (Young et al, 2012). It is important to address contact lens-related discomfort, dryness, and dryness-induced vision issues, as these can all be factors that contribute to patients discontinuing contact lens wear (Valencia-Nieto et al, 2023).
In this case, the patient was advised to start consistently removing makeup nightly with appropriate makeup removers, apply warm compresses nightly with a heated eyelid mask, and use an appropriate contact lens artificial tear during prolonged screen use. Lastly, the patient was educated on the importance of consistency in treatment. At her second follow-up after starting the above treatments, she was wearing the same lenses initially dispensed, her symptoms were resolved, and her vision was stable.
Before we fit our patients in any contact lens, it’s important to carefully inspect their ocular surface, lid margins, lashes, and meibomian glands and identify any issues. Another area to consider is their skin-care and makeup routine and how they apply and remove makeup around the eyes. Starting a consistent treatment regimen before initiating contact lens wear can significantly impact the patient’s success and their perception of how well their contact lenses are working.
REFERENCES
1. Stapleton F, Bakkar M, Carnt N, et al. CLEAR - Contact lens complications. Cont Lens Anterior Eye. 2021 Apr;44:330-367.
2. Young G, Chalmers R, Napier L, Kern J, Hunt C, Dumbleton K. Soft contact lens-related dryness with and without clinical signs. Optom Vis Sci. 2012 Aug;89:1125-1132.
3. Valencia-Nieto L, López-de la Rosa A, López-Miguel A, González-García MJ. Clinical characterisation of contact lens discomfort progression. Cont Lens Anterior Eye. 2023 Dec 13:102096.