


This article was originally published in a sponsored newsletter.
Orthokeratology (ortho-k) lenses are traditionally fit based on a patient’s keratometry values and refraction. Using these initial values, practitioners are able to select an initial base curve while accounting for a desired Jessen factor. Keratometry readings are also traditionally used to determine the initial reverse curve depth and alignment zone(s). Thresholds for toric lens design vary depending on the lens design. Additional data that labs may use is corneal elevation or corneal toricity data at an 8mm chord to determine whether a toric lens design is required.1,2
Another piece of information that has become increasingly helpful when fitting ortho-k is a patient’s corneal diameter. While most ortho-k lenses traditionally used standard overall diameters, considering the patient’s corneal diameter may suggest a more customized diameter instead.
When fitting ortho-k, an ideal fluorescein pattern has a centered, round treatment zone over the pupil with a round fluorescein-filled reverse curve. Beyond the reverse curve, the lens should be aligned 360º with an adequate edge clearance. Ideally, there should be around 1mm of movement, but this may vary depending on the design. Although a fluorescein pattern may look ideal in an open-eye environment, that does not indicate how the lens centers and performs on the eye while the patient is asleep.
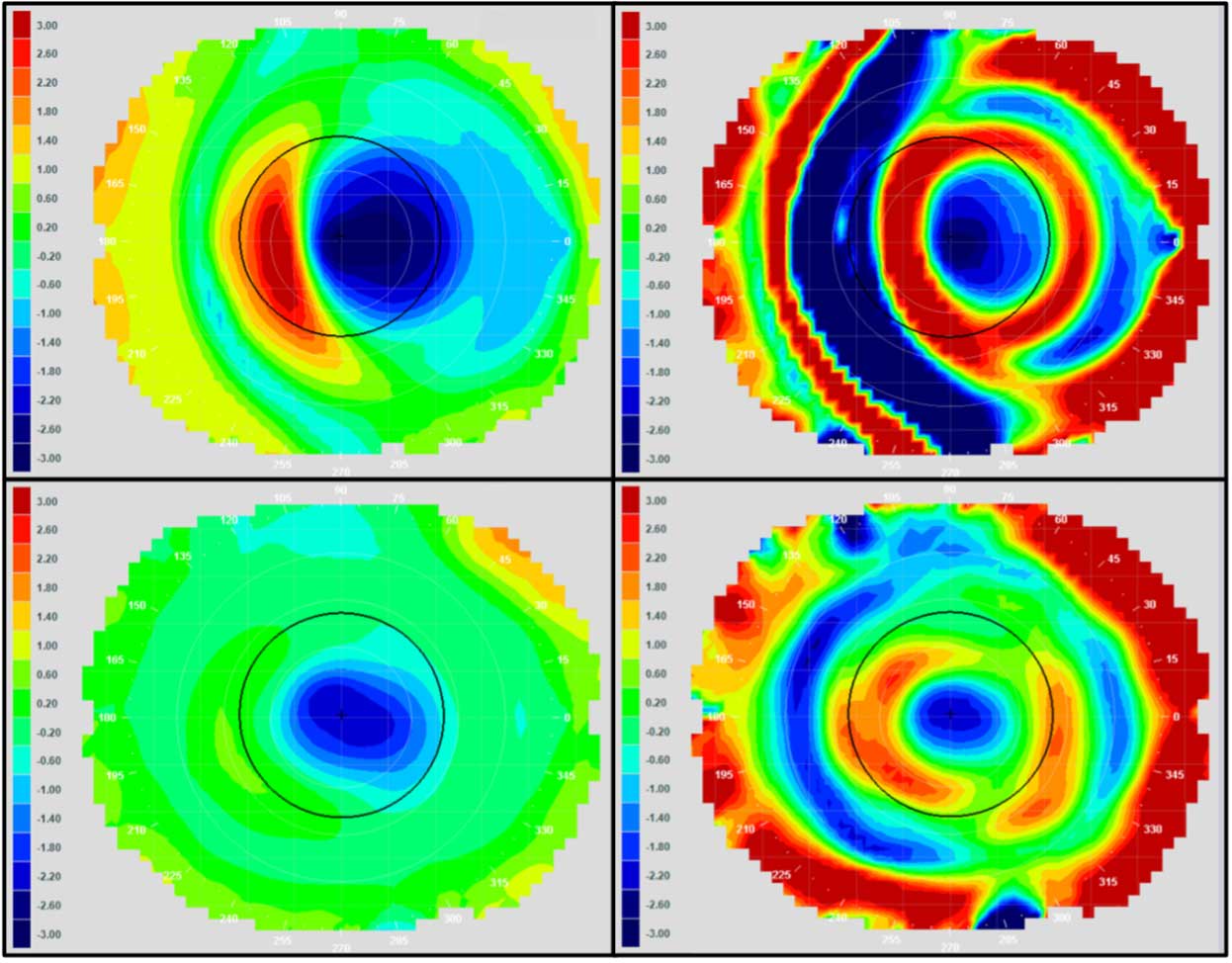
Topography is a useful tool for analyzing the lens centration and performance in a closed-eye environment. Topography allows practitioners to view lens centration and treatment that occurs while the patient is sleeping. Ideally, the topography reveals a “red ring” centered around the pupil indicating midperipheral steepening in the reverse curve area and flattening in the central treatment zone; however, this is not always the case, and fit changes may be indicated to improve centration.
When troubleshooting fit changes in ortho-k, moving to a larger overall diameter often improves lens centration. This is most often considered with lateral decentration, but also helpful with superior and inferior decentration as well.1
Also, a larger overall diameter is typically more comfortable for the patient. While this change may be made later on in the fit process, knowing the patient’s corneal diameter during initial lens design is helpful to incorporate a larger diameter, if needed.
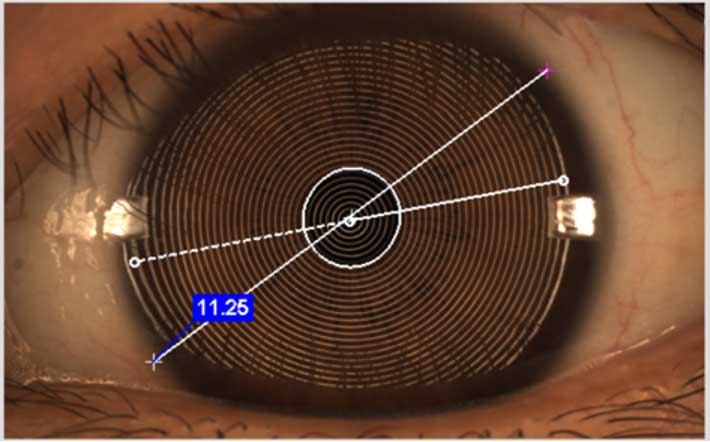
The corneal diameter is most accurately measured using a corneal topographer. Measurement techniques may vary depending on the device used. Some topographers automatically measure the horizontal visible iris diameter (HVID); others measure the diagonal visible iris diameter (DVID). Since most corneas are not perfectly round, with the HVID typically larger than the vertical visible iris diameter (VVID), the DVID tends to be slightly smaller than a true horizontal measurement.
Horizontal measurements may also differ between instruments. While HVID and horizontal white to white (HWTW) are typically used interchangeably, there is a slight difference in which landmarks are used to acquire each measurement. HVID is the visible width of the iris, while HWTW is typically a slightly larger measurement and extends from limbus to limbus.3 Most topographers use the photo taken of the iris and measure from white to white. Some topographers will do this automatically, while others require the practitioner to do this manually. If the topography image does not capture both sides of the cornea along the horizontal plane, a DVID measurement may be taken at around a 45º angle.
Philosophies on diameter selection may vary depending on the lens design. Some manufacturers recommend covering a certain percentage of the cornea (such as 90%) and others may recommend an overall diameter that is smaller than the corneal diameter by a standard amount (such as 0.8mm). Depending on the design, more or less coverage may be recommended. Discussion of parameter selection with a manufacturer’s consultation department is helpful to learn more about each specific lens design and recommendations.
Fitting ortho-k lenses has become increasingly guided by software. Although there is still the option of fitting ortho-k empirically using a diagnostic fitting set, topography-guided designs allow for further customization of lens parameter options, often with better success during a fitting process. True software-guided designs also may allow fitting patients who may be more difficult, such as in the case of against-the-rule astigmatism or high amounts of corneal toricity and may also use corneal diameter as a helpful tool to suggest a larger initial diameter. These advancements in technology emphasize the importance of topography with ortho-k fitting success.
Keratometry values and refraction remain the bread and butter of ortho-k fitting. However, with advancements in technology and lens design, additional data points provided by topography have proven increasingly helpful.
References:
- Vincent SJ, Cho P, Chan KY, et al. BCLA CLEAR-Orthokeratology. Cont Lens Anterior Eye. 2021 Apr;44:240-269.
- Zhang L, Zhang Y, Liu Y, Wang K, Zhao M. A novel fitting algorithm for alignment curve radius estimation using corneal elevation data in orthokeratology lens trial. Cont Lens Anterior Eye. 2017 Dec;40:401-407.
- Bergmanson JP, Martinez JG. Size does matter: what is the corneo‐limbal diameter? Clin Exp Optom. 2017 Sep;100:522-528.
