


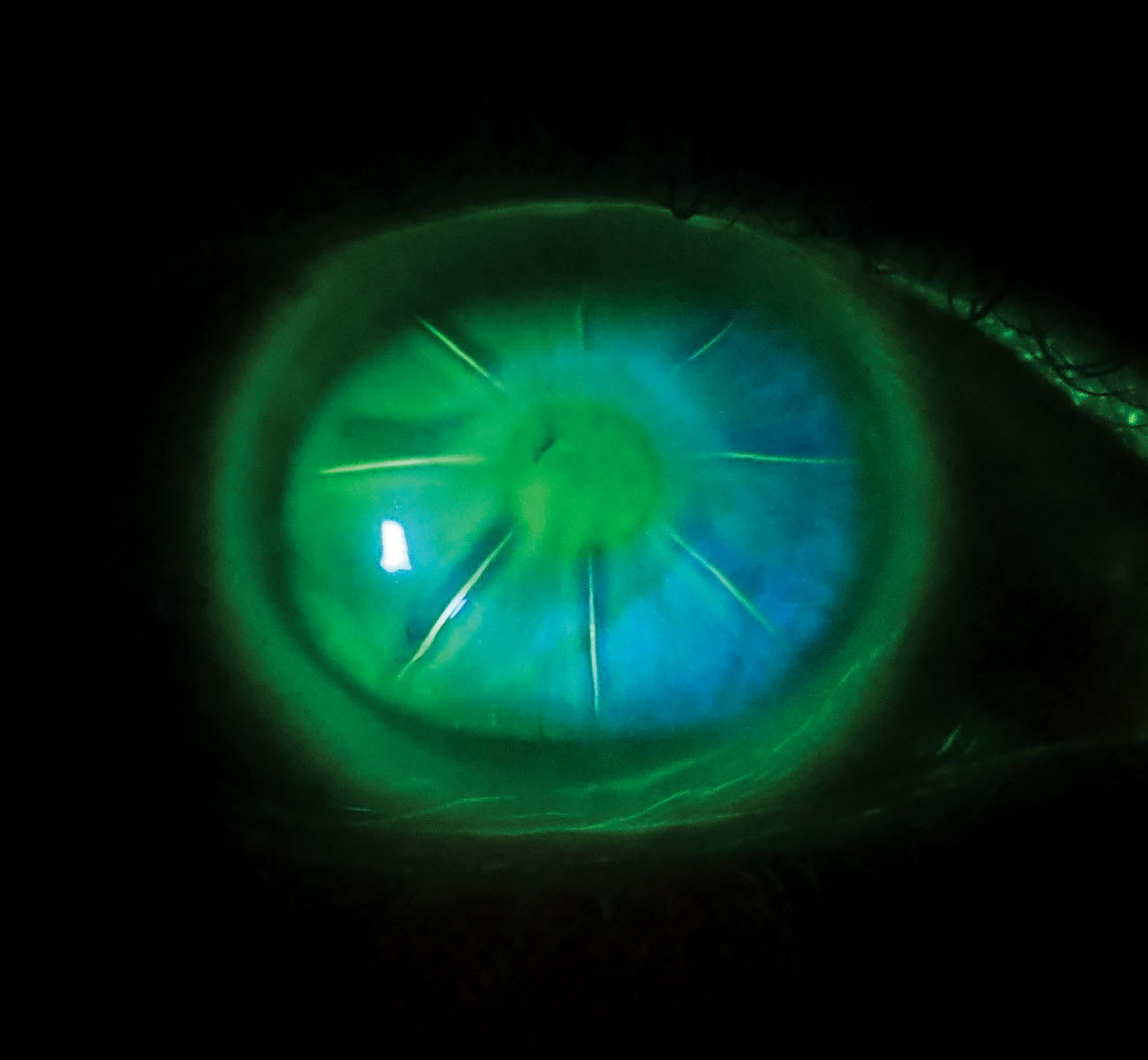
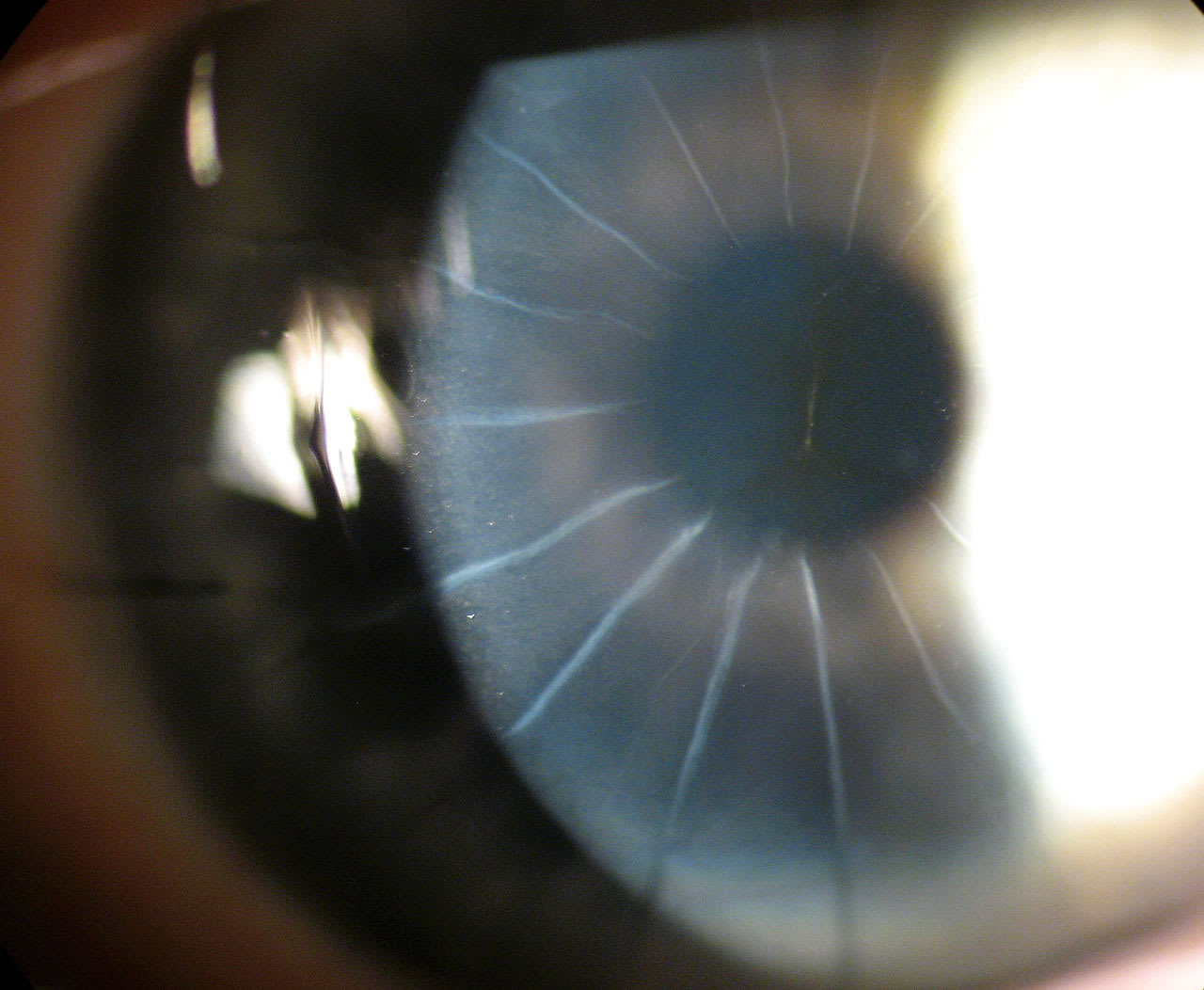
ALTHOUGH RADIAL keratotomy (RK) was eventually eclipsed by laser vision correction, 250,000 RK procedures were performed annually at the peak of its popularity in the early 1990s for the correction of myopia (National Eye Institute, 1994). The surgery involved making 4 to 32 (sometimes more!) deep radial corneal incision (Figures 1 and 2) that resulted in corneal flattening. Three-year results of the Prospective Evaluation of Radial Keratotomy (PERK) study showed that 58% of eyes had refractive error within 1.00 D of emmetropia, 26% were undercorrected, and 16% were overcorrected by more than 1.00 D (Waring et al, 1987).
Postoperative RK patients can develop irregular astigmatism, corneal ectasia, and refractive fluctuations with change in altitude (Mader et al, 1995). Approximately 60% of patients complain of diurnal vision fluctuations; most of them shift toward myopia (Chang et al, 2025; Schanzlin et al, 1987). A study by MacRae and colleagues (1989) evaluated 8 patients 2 weeks after RK surgery and found that the treated eyes were on average 1.48 D more hyperopic in the morning as compared to the afternoon visit 8 hours later.
This is a case report of a post-RK patient who had significant diurnal refractive fluctuations and was successfully managed with scleral lenses.
A 64-year-old female patient post RK surgery in both eyes has a 20-year history of diurnal refractive fluctuations with glasses prescriptions. A recent morning manifest refraction was +5.00 –2.00 x 096 20/20 OD and +6.75 –1.75 x 049 20/20 OS. Her afternoon manifest refraction was +7.50 –2.75 x 98 20/20 OD and +7.25 –2.00 x 061 20/20 OS.
Slit lamp examination showed 8-incision RK in each eye, without additional scarring or neovascularization. The patient habitually wears scleral lenses that provide her stable vision without any diurnal fluctuations. The lenses had parameters of 16.5 mm diameter, base curve (BC) of 37.5 D (sag 4525 µm), and toric landing zone 241 µm, +2.25 20/20 OD; and 16.0 mm diameter, BC of 41.75 D (sag 4318 µm), and toric landing zone 196 microns, –3.37 20/25 OS. The Dk of the lens material was 180.
She typically wears scleral lenses, but on the days that she chooses not to wear her scleral lenses, she switches pairs of glasses from morning to afternoon.
Although diurnal fluctuations are relatively common, this patient is unique in that her refractive shift is in the hyperopic rather than the myopic direction. Typically, RK patients wear scleral lenses for the primary purpose of improving vision secondary to irregular astigmatism. For this patient, customized scleral lenses not only successfully fit her eyes despite her significant oblate corneal surface, but also gave her the benefit of diurnal refractive stabilization during lens wear. There has been at least 1 case report of the use of soft lenses to stabilize diurnal fluctuations. A paper by Inoue and colleagues (2020) described a patient with –1.80 D diurnal fluctuations that were minimized to 0.50 D using high-Dk soft contact lens wear. Interestingly, the patient had a 2.3 D hyperopic change with low-Dk soft lenses. Corneal cross-linking also shows promise for mitigating diurnal fluctuations secondary to RK; however, a hyperopic shift tends to occur post treatment (Elbaz et al, 2014).
References
1. National Eye Institute. Ten-year results on radial keratotomy released. October 13, 1994. Accessed May 9, 2025. nei.nih.gov/about/news-and-events/news/ten-year-results-radial-keratotomy-released
2. Waring GO 3rd, Lynn MJ, Culbertson W, et al. Three-year results of the Prospective Evaluation of Radial Keratotomy (PERK) Study. Ophthalmology. 1987 Oct;94(10):1339-54. doi: 10.1016/s0161-6420(87)80021-0
3. Mader TH, White LJ. Refractive changes at extreme altitude after radial keratotomy. Am J Ophthalmol. 1995 Jun;119(6):733-7. doi: 10.1016/s0002-9394(14)72777-1
4. Chang V, Bunya VY, Lizarraga MT. Radial keratotomy: complications management. EyeWiki American Academy of Ophthalmology. May 9, 2025. Accessed May 9, 2025. eyewiki.org/Radial_Keratotomy:_Complications_Management
5. Schanzlin DJ, Santos VR, Waring GO 3rd, et al. Diurnal change in refraction, corneal curvature, visual acuity, and intraocular pressure after radial keratotomy in the PERK Study. Ophthalmology. 1986;93(2):167-75. doi: 10.1016/s0161-6420(86)33765-5
6. McRae S, Rich L, Phillips D, Bedrossian R. Diurnal variation in vision after radial keratotomy. Am J Ophthalmol. 1989;107(3):262-267. doi: 10.1016/0002-9394(89)90310-3
7. Inoue T, Maeda N, Inoue Y, Shimomura Y, Tano Y. Minimizing radial-keratotomy-induced diurnal variation in vision using contact lenses. J Cataract Refract Surg. 2000;26(11):1680-3. doi: 10.1016/s0886-3350(00)00718-5
8. Elbaz U, Yeung SN, Ziai S, et al. Collagen crosslinking after radial keratotomy. Cornea. 2014;33(2):131-6. doi: 10.1097/ICO.0000000000000044