


LEARNING METHOD AND MEDIUM
This educational activity consists of a written article and 20 study questions. The participant should, in order, read the Activity Description listed at the beginning of this activity, read the material, answer all questions in the post test, and then complete the Activity Evaluation/Credit Request form. To receive credit for this activity, please follow the instructions provided below in the section titled To Obtain CE Credit. This educational activity should take a maximum of two hours to complete.
CONTENT SOURCE
This continuing education (CE) activity captures key statistics and insights from contributing
faculty.
ACTIVITY DESCRIPTION
In this article, learners will explore the latest evidence-based information related to current and future myopia management strategies, and learn about resources that can help them effectively slow myopia progression and enhance the care of young myopic patients.
TARGET AUDIENCE
This educational activity is intended for optometrists, contact lens specialists, and other eyecare professionals.
ACCREDITATION DESIGNATION STATEMENT
This course is COPE accredited for two hours of CE credit. COPE Course ID: 95904-GO
DISCLOSURES
Jeffrey J. Walline, OD, PhD, reports no conflicts of interest.
DISCLOSURE ATTESTATION
The contributing faculty member has attested to the following:
1. That the relationships/affiliations noted will not bias or otherwise influence his involvement in this activity;
2. That practice recommendations given relevant to the companies with whom he has relationships/affiliations will be supported by the best available evidence or, absent evidence, will be consistent with generally accepted medical practice;
3. That all reasonable clinical alternatives will be discussed when making practice recommendations.
TO OBTAIN CE CREDIT
To obtain COPE CE credit for this activity, read the material in its entirety and consult referenced sources as necessary. We offer instant certificate processing for COPE credit. Please take the post test and evaluation online by using your OE tracker number and logging in to visioncarece.com.
Upon passing the test, you will immediately receive a printable PDF version of your course certificate for COPE credit. On the last day of the month, your course results will be forwarded to ARBO with your OE tracker number, and your records will be updated. You must score 70% or higher to receive credit for this activity. Please make sure that you take the online post test and evaluation on a device that has printing capabilities.
NO-FEE CONTINUING EDUCATION
There are no fees for participating in and receiving credit for this CE activity.
Disclaimer
The views and opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of Contact Lens Spectrum. This activity is copyrighted to Conexiant ©2025. All rights reserved.
CE Questions? Contact accred@conexianteducation.com for help.
Release date: MARCH 1, 2025
Expiration Date: JANUARY 21, 2028
MYOPIA MANAGEMENT is rapidly evolving and should be of particular interest to all eyecare practitioners who examine young myopic patients. Myopia is finally being recognized as a disease1 for which we should provide treatments that manage the mechanism of progression, as opposed to simply alleviating the symptoms. The argument can be made that for young myopic children, the new standard of care consists of myopia management strategies, not single-vision correction of blurry distance vision. It is imperative that eyecare practitioners arm themselves with as much knowledge as possible about the rapidly advancing treatment strategies, and there are several ways to accomplish that.
This article teaches ECPs about the basics of myopia control, provides evidence-based information about myopia management advances, and answers many questions that both experienced and novice myopia control practitioners may ask.
RESOURCES
It is imperative that practitioners know the most up-to-date information about myopia control, because that information is available to the parents of our patients as well. Physicians should demonstrate their expertise by being familiar with the current evidence and providing patients with answers to their questions. This article offers some resources to help practitioners to remain current with their information.
The National Academies of Science, Engineering, and Medicine published Myopia: Causes, Prevention, and Treatment of an Increasingly Common Disease.1 This publication provides eyecare clinicians with balanced, evidence-based theories about the increase in myopia prevalence and strategies to combat it. It also provides a strong basis for advocacy efforts to obtain myopia management coverage via insurance.
Eyecare practitioners should also attend myopia management continuing education seminars, critically evaluate the scientific literature, read the International Myopia Institute (IMI) papers that provide important myopia management updates every two years (myopiainstitute.org), and read the great summaries of the latest information in Myopia Profile (myopiaprofile.com). The IMI paper topics range from genetics to clinical management guidelines. The information is compiled from the peer-reviewed literature by experts in the field and made available to everyone.
Myopia Profile is edited by practitioners from Australia. They travel the world to keep abreast of the newest research, and they compile it in easy-to-read summaries. They also have a Facebook page where providers can ask questions and obtain feedback from other myopia control colleagues from around the world. Some ask about difficult patients they manage, while others ask about the latest research.
All of these resources—and many more—provide excellent information that allows eyecare practitioners to practice at the highest level to reduce the burden of myopia.
CURRENT TREATMENT OPTIONS
In the U.S., there are three current treatment modalities available to practitioners: center-distance soft multifocal contact lenses, orthokeratology, and low-concentration atropine. Let’s discuss each, including some new information.
Soft Multifocal Contact Lenses The only contact lens modality that the U.S. Food and Drug Administration (FDA) has cleared for myopia control is soft multifocal contact lenses.2 However, other modalities can be used off-label for myopia control without fear of additional liability, as long as there is scientific evidence to indicate that they can also control myopia.3 So far, only soft multifocals with a center-distance design have been investigated for myopia control, so those lenses with a center-near design should not be used for myopia control.
The putative cue for soft multifocal contact lens myopia control has long been reported to be the amount of peripheral myopic defocus, but results from the Bifocal Lenses In Nearsighted Kids (BLINK) study indicated that there is not a dose-response relationship between the amount of peripheral myopic defocus and slower eye growth and posits that something else, such as peripheral image quality, explains the majority of the benefit.4 The BLINK study also showed that accommodative response is less while the patient is wearing the lenses, but nearly five years of multifocal contact lens wear did not negatively affect accommodative amplitudes, facility, or lag.5
Another study indicated that six years of treatment with a dual-focus lens resulted in 0.52mm slower eye growth than when treated with single-vision contact lenses, and that the amount of eye growth is similar to that expected of emmetropic eyes.6
In summary, soft multifocal contact lenses slow myopia progression and eye growth, but it is unlikely that the amount of myopic defocus is related to the amount of slowing. While soft multifocal contact lenses don’t stop myopia progression, they do slow eye growth to a rate that is similar to emmetropic eye growth—and they do so without harming the accommodative system in children.
Orthokeratology Orthokeratology effectively slows myopia progression,7 and it is the only treatment that has been investigated for myopia control in highly myopic patients8 and patients who have significant astigmatism.9
Two randomized clinical trials recently indicated that smaller treatment zones provided better myopia control,10,11 but also decreased objective visual quality10,11 without affecting subjective visual quality.11 These results indicate that greater defocus or poor image quality in the periphery may explain the myopia control benefits of orthokeratology contact lens wearers.
Low-Concentration Atropine Until recently, all low-concentration atropine studies were conducted in Asia, and they indicated that nightly administration of concentrations as low as 0.01% effectively slowed the progression of myopia, although the slowing of eye growth may not have been as effective at the lowest concentrations.
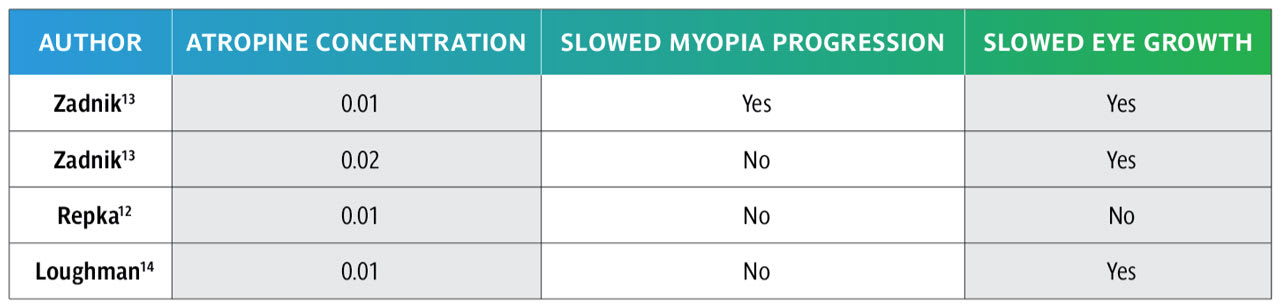
Recent randomized clinical trials conducted in primarily Caucasian samples indicated that evidence of nightly administration of the lowest concentrations of atropine is relatively unclear, probably indicating that the treatment isn’t as potent as practitioners would like.12-14 The Childhood Atropine for Myopia Progression (CHAMP) study reported that 0.01% atropine slowed myopia progression and eye growth and increased the proportion of participants who progressed less than –0.50D over three years. However, 0.02% did not slow myopia progression or increase the proportion of participants who progressed less than –0.50D over three years, but it did slow eye growth.13 The Myopia Treatment Study (MTS) reported that 0.01% atropine did not slow myopia progression or eye growth.12 The Myopia Outcome Study of Atropine in Children (MOSAIC) reported that 0.01% atropine slowed eye growth but not myopia progression over two years.14 Results of the studies are summarized in Table 1.
Red Light Therapy Two three-minute sessions separated by at least four hours of red light therapy slows myopia progression and eye growth,15-18 but it isn’t available in the U.S. Recent studies indicate that discontinuation of red light therapy may lead to loss of treatment effect secondary to the rebound effect.17,19 A recent study also indicated that the therapy may photochemically and thermally damage the retina,20 as indicated by a case reported of irreversible vision loss following red light therapy.21 While this therapy may initially exhibit a large treatment effect—even a regression of myopia and eye length—caution is warranted due to significant rebound effects and the potential for retinal damage.
Myopia Control Spectacles Currently, there aren’t any spectacle lenses available in the U.S. that provide evidence-based effective myopia control. However, there have been several investigations of specific myopia control spectacles that either incorporate lenslets with relative plus power in the peripheral lens22-25 or decrease contrast to the peripheral retina,26 and they all exhibited meaningful myopia control. The timeline for potential FDA approval of a spectacle-based indication for myopia control is unknown.
Although there haven’t been any long-term studies of the rebound effect after discontinuing myopia control spectacles, discontinuation doesn’t appear to meaningfully increase myopia progression or eye growth.27,28 Myopia progression and eye growth both speed up after changing to single-vision correction, but the rate of change is not enough to eliminate the treatment effect in a relatively short period of time.27
Combination Treatment Several combination therapies were investigated to determine whether they provided better myopia control than monotherapy29-32 (Table 2). Only a combination of soft multifocal contact lenses and 0.01% atropine showed no statistically significant effect, but the difference in eye growth between the combination therapy and monotherapy was similar for soft multifocal contact lenses31 and orthokeratology,29,30 indicating that soft multifocal contact lenses may also be used in combination with atropine to provide additional myopia control benefit if monotherapy alone does not seem to provide a meaningful effect.
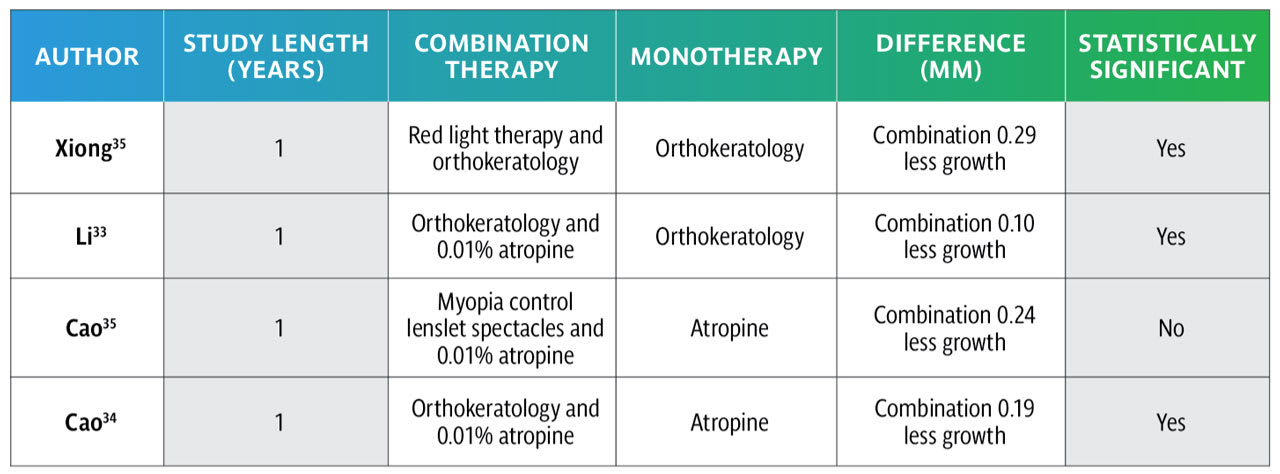
Recently, combining a pharmaceutical treatment with an optical treatment significantly slowed eye growth over a one-year period when compared to orthokeratology lenses alone33 or atropine alone.34 Similarly, combining red light therapy and orthokeratology slowed eye growth more than orthokeratology alone for people who exhibited fast eye growth while wearing orthokeratology alone.35 Overall, if a single treatment does not seem to provide sufficient myopia management, then adding a second treatment is likely to provide additional benefit.
REBOUND
A systematic review indicated that optical treatments such as soft multifocal contact lenses, orthokeratology, and lenslet spectacles may result in less rebound effect than atropine or low-level red light therapy.36 Another review paper examined rebound with a variety of treatment modalities, and the authors reported that soft contact lenses, myopia control spectacles, and < 0.1% atropine showed no rebound, but orthokeratology, ≥ 0.1% atropine, and red light therapy exhibited statistically significant rebound.37 The Western Australia–Atropine for the Treatment of Myopia (WA-ATOM) study indicated that, after two years of treatment with 0.01% atropine, one year of discontinuation resulted in faster myopia progression and eye growth than the placebo group, which negated the initial treatment effect while on 0.01% atropine.38
DELAYING MYOPIA ONSET
A randomized clinical trial provided evidence that 0.05% atropine administered nightly—but not 0.01% atropine—can decrease the two-year incidence of myopia onset from 54% to 28% when compared to placebo.39 The 0.05% atropine eye drops also reduced the myopic shift and eye growth compared to placebo and decreased the proportion of participants who exhibited at least a 1D myopic shift from 54% to 25%. The delayed onset was achieved without any increase in adverse events or decrease in quality of life.39
However, young pre-myopic patients are unlikely to report for routine eye examinations unless their siblings have myopia, so if practitioners want to have a meaningful effect in delaying the onset of myopia, they may need to predict which children are most likely to become myopic. They can do this relatively easily and effectively solely by measuring the cycloplegic refractive error of young children; even including other ocular component measures doesn’t improve the predictive ability of myopia onset.40 Table 3 indicates the most hyperopic cycloplegic spherical equivalent refractive error cutpoints by age that predict the onset of myopia by age 13.
Children who have refractive errors less hyperopic than those indicated for each age in Table 3 are the ones who will most likely benefit from delayed myopia onset.

PREDICTING MYOPIA PROGRESSION
Many practitioners only provide myopia management information if a child exhibits significant progression during the previous year, so investigators conducted a study to determine whether one year of myopia progression or eye growth predicts faster progression or eye growth during the subsequent year.41 They found that the first year of progression explains only about 1.5% of the variance in the second year of progression, and the first year of eye growth provides no value in determining the second. That indicates that eyecare practitioners should provide myopia management to all young myopic patients rather than only to those who progress “quickly.”
UNDERSTANDING WHO RESPONDS TO TREATMENT
Similar to difficulty predicting the following year of myopia progression, it is also difficult to differentiate between children who exhibit a meaningful treatment effect (“responders”) and those who do not (“nonresponders”). Brennan and colleagues analyzed data from the Low-Concentration Atropine for Myopia Progression (LAMP) study, and they showed that the average difference in progression between treated and control groups was the same, regardless of the rate of progression, so practitioners cannot assume that fast progressors are poor responders and slow progressors are strong responders. Thus, practitioners should add a second therapy only if they or the parents are anxious, rather than adding a treatment based on the rate of progression of the individual child.
SCREEN TIME
Several previously conducted systematic reviews reported conflicting results as to whether screen time was associated with myopia, so Zong and colleagues provided an updated assessment of the effects of screen time on myopia.42 When categorizing screen time into high versus low amounts of screen time, results indicated more than double the risk of being myopic, regardless of whether it was a cross-sectional or longitudinal study. Using a continuous measure of screen time showed only a 7% increased risk of being myopic for every additional hour of screen time in longitudinal studies, but no association was observed for cross-sectional studies. Furthermore, sensitivity analysis indicated that only the cross-sectional categorization of screen, not longitudinal, time resulted in a significant effect.42
The authors concluded, “Screen time exposure was significantly associated with myopia in children and adolescents.”42However, when you consider that only cross-sectional categorization of screen time exhibited a meaningful association and cross-sectional results imply association, not causation, it is unlikely that screen time has a meaningful effect on the onset of myopia.
MYOPIA PREVALENCE AND COST
It was previously estimated that half of the world’s population would be myopic and 10% of the population would be highly myopic by 2050.43 A more recent publication predicts a 40% global and 35% North American prevalence of myopia by 2050.44 Regardless of the actual prevalence of myopia, it is a disease that affects an extremely high proportion of people. So, in the United States, the annual cost of eye examinations and single-vision correction for poor distance vision is between $7.3 and $13.5 billion, when adjusted for inflation.45
We must, as practitioners, begin to treat the disease and not just alleviate the symptoms. That is the only way we will be able to reduce the burden myopia puts on society and the associated monetary and ocular health effects it has on individuals.
REFERENCES
1. National Academies of Sciences, Engineering, and Medicine. Myopia: Causes, Prevention, and Treatment of an Increasingly Common Disease. The National Academies Press. 2024.
2. Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom Vis Sci. 2019 Aug;96:556-567.
3. Walline JJ, Walker MK, Mutti DO, et al; BLINK Study Group. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA. 2020 Aug 11;324:571-580.
4. Berntsen DA, Ticak A, Sinnott LT, et al; BLINK Study Group. Peripheral Defocus, Pupil Size, and Axial Eye Growth in Children Wearing Soft Multifocal Contact Lenses in the BLINK Study. Invest Ophthalmol Vis Sci. 2023 Nov 1;64:3.
5. Chandler MA, Robich ML, Jordan LA, et al; BLINK2 Study Group. Accommodation in Children after 4.7 Years of Multifocal Contact Lens Wear in the BLINK Study Randomized Clinical Trial. Optom Vis Sci. 2023 Jul 1;100:425-431.
6. Chamberlain P, Hammond DS, Arumugam B, Bradley A. Six-year cumulative treatment effect and treatment efficacy of a dual focus myopia control contact lens. Ophthalmic Physiol Opt. 2024 Jan;44:199-205.
7. Cho P, Cheung SW. Retardation of myopia in orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012 Oct 11;53:7077-7085.
8. Charm J, Cho P. High Myopia-Partial Reduction Ortho-k: A 2-Year Randomized Study. Optom Vis Sci. 2013 Jun;90:530-539.
9. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res. 2005 Jan;30:71-80.
10. Tang WT, Luo XN, Zhao WJ, et al. One-year results for myopia control of orthokeratology with different back optic zone diameters: a randomized trial using a novel multispectral-based topographer. Int J Ophthalmol. 2024 Feb 18;17:324-330.
11. Gong G, Zhang BN, Guo T, et al. Efficacy of orthokeratology lens with the modified small treatment zone on myopia progression and visual quality: a randomized clinical trial. Eye Vis (Lond). 2024 Sep 2;11:35.
12. Repka MX, Weise KK, Chandler DL, et al. Low-Dose 0.01% Atropine Eye Drops vs Placebo for Myopia Control: A Randomized Clinical Trial. JAMA Ophthalmol. 2023 Aug 1;141:756-765.
13. Zadnik K, Schulman E, Flitcroft I, et al. Efficacy and Safety of 0.01% and 0.02% Atropine for the Treatment of Pediatric Myopia Progression Over 3 Years: A Randomized Clinical Trial. JAMA Ophthalmol. 2023 Oct 1;141:990-999.
14. Loughman J, Kobia-Acquah E, Lingham G, et al. Myopia outcome study of atropine in children: Two-year result of daily 0.01% atropine in a European population. Acta Ophthalmol. 2024 May;102(3):e245-e256.
15. Zhou L, Xing C, Qiang W, Hua C, Tong L. Low-intensity, long-wavelength red light slows the progression of myopia in children: an Eastern China-based cohort. Ophthalmic Physiol Opt. 2022 Mar;42:335-344.
16. Jiang Y, Zhu Z, Tan X, et al. Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children. Ophthalmology. 2022 May;129:509-519.
17. Chen H, Wang W, Liao Y, et al. Low-intensity red-light therapy in slowing myopic progression and the rebound effect after its cessation in Chinese children: a randomized controlled trial. Graefes Arch Clin Exp Ophthalmol. 2023 Feb;261:575-584.
18. Liu Y, Zhu M, Yan X, Li M, Xiang Y. The Effect of Repeated Low-Level Red-Light Therapy on Myopia Control and Choroid. Transl Vis Sci Technol. 2024 Oct 1;13:29.
19. Xiong R, Zhu Z, Jiang Y, et al. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clin Exp Ophthalmol. 2022 Dec;50:1013-1024.
20. Ostrin LA, Schill AW. Red light instruments for myopia exceed safety limits. Ophthalmic Physiol Opt. 2024 Mar;44:241-248.
21. Liu H, Yang Y, Guo J, Peng J, Zhao P. Retinal Damage After Repeated Low-level Red-Light Laser Exposure. JAMA Ophthalmol. 2023 Jul 1;141:693-695.
22. Zhang Z, Zeng L, Gu D, et al. Spectacle Lenses With Highly Aspherical Lenslets for Slowing Axial Elongation and Refractive Change in Low-Hyperopic Chinese Children: A Randomized Controlled Trial. Am J Ophthalmol. 2024 Aug 27;269:60-68.
23. Bao J, Huang Y, Li X, et al. Spectacle Lenses With Aspherical Lenslets for Myopia Control vs Single-Vision Spectacle Lenses: A Randomized Clinical Trial. JAMA Ophthalmol. 2022 May 1;140:472-478.
24. Lam CS, Tang WC, Lee PH, et al. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: results of a 3-year follow-up study. Br J Ophthalmol. 2022 Aug;106:1110-1114.
25. Su B, Cho P, Vincent SJ, et al. Novel Lenslet-ARray-Integrated Spectacle Lenses for Myopia Control: A 1-Year Randomized, Double-Masked, Controlled Trial. Ophthalmology. 2024 Dec;131:1389-1397.
26. Rappon J, Chung C, Young G, et al. Control of myopia using diffusion optics spectacle lenses: 12-month results of a randomised controlled, efficacy and safety study (CYPRESS). Br J Ophthalmol. 2023 Nov;107:1709-1715.
27. Lam CSY, Tang WC, Zhang HY, et al. Long-term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years. Sci Rep. 2023 Apr 4;13:5475.
28. Sankaridurg P, Weng R, Tran H, et al. Spectacle Lenses With Highly Aspherical Lenslets for Slowing Myopia: A Randomized, Double-Blind, Cross-Over Clinical Trial: Parts of these data were presented as a poster at the Annual Research in Vision and Ophthalmology meeting, 2022. Am J Ophthalmol. 2023 Mar;247:18-24.
29. Kinoshita N, Konno Y, Hamada N, et al. Efficacy of combined orthokeratology and 0.01% atropine solution for slowing axial elongation in children with myopia: a 2-year randomised trial. Sci Rep. 2020 Jul 29;10:12750.
30. Tan Q, Ng AL, Choy BN, Cheng GP, Woo VC, Cho P. One-year results of 0.01% atropine with orthokeratology (AOK) study: a randomised clinical trial. Ophthalmic Physiol Opt. 2020 Aug 10;40:557-566.
31. Jones J, Mutti D, Jones-Jordan L, Walline J. Effect of Combining 0.01% Atropine with Soft Multifocal Contact Lenses on Myopia Progression in Children. Optom Vis Sci. 2022 May 1;99:434-442.
32. Huang Z, Chen XF, He T, Tang Y, Du CX. Synergistic effects of defocus-incorporated multiple segments and atropine in slowing the progression of myopia. Sci Rep. 2022 Dec 24;12:22311.
33. Li B, Yu S, Gao S, et al. Effect of 0.01% atropine combined with orthokeratology lens on axial elongation: a 2-year randomized, double-masked, placebo-controlled, cross-over trial. Front Med (Lausanne). 2024 Apr 23;11:1358046.
34. Cao X, Guo Z, Wei Z, et al. Effect of 0.01% atropine eye drops combined with different optical treatments to control low myopia in Chinese children. Cont Lens Anterior Eye. 2024 Oct 16:102317.
35. Xiong R, Wang W, Tang X, et al. Myopia Control Effect of Repeated Low-Level Red-Light Therapy Combined with Orthokeratology: A Multicenter Randomized Controlled Trial. Ophthalmology. 2024 Nov;131:1304-1313.
36. Sanchez-Tena MA, Ballesteros-Sanchez A, Martinez-Perez C, et al. Assessing the rebound phenomenon in different myopia control treatments: A systematic review. Ophthalmic Physiol Opt. 2024 Mar;44:270-279.
37. Bullimore MA, Brennan NA. Efficacy in myopia control-The impact of rebound. Ophthalmic Physiol Opt. 2025 Jan;45:100-110.
38. Lee SSY, Nilagiri VK, Lingham G, et al. Myopia progression following 0.01% atropine cessation in Australian children: Findings from the Western Australia – Atropine for the Treatment of Myopia (WA-ATOM) study. Clin Exp Ophthalmol. 2024 Jul;52:507-515.
39. Yam JC, Zhang XJ, Zhang Y, et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children: The LAMP2 Randomized Clinical Trial. JAMA. 2023 Feb 14;329(6):472-481.
40. Zadnik K, Sinnott LT, Cotter SA, et al; Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) Study Group. Prediction of Juvenile-Onset Myopia. JAMA Ophthalmol. 2015 Jun;133:683-689.
41. Mutti DO, Sinnott LT, Brennan NA, et al; Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) Study Group. The Limited Value of Prior Change in Predicting Future Progression of Juvenile-onset Myopia. Optom Vis Sci. 2022. May 1;99:424-433.
42. Zong Z, Zhang Y, Qiao J, Tian Y, Xu S. The association between screen time exposure and myopia in children and adolescents: a meta-analysis. BMC Public Health. 2024 Jun 18;24:1625.
43. Holden BA, Fricke TR, Wilson DA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016 May;123:1036-42.
44. Liang J, Pu Y, Chen J, et al. Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br J Ophthalmol. 2024 Sep 24;bjo-2024-325427.
45. Vitale S, Cotch MF, Sperduto R, Ellwein L. Costs of refractive correction of distance vision impairment in the United States, 1999-2002. Ophthalmology. 2006 Dec;113:2163-2170.