


ORTHOKERATOLOGY (ortho-k) offers a myriad of advantages to patients, serving as a reversible, nonsurgical alternative for vision correction and an excellent option for those seeking freedom from daytime correction. However, ortho-k’s most compelling benefit lies in its ability to slow the progression of myopia. By addressing both immediate visual needs and long-term ocular health, ortho-k not only enhances daily life but also plays a crucial role in mitigating the risks associated with progressive myopia, making it a truly transformative solution for patients.
The reverse geometry design of ortho-k lenses creates central flattening that reduces myopic refractive error and mid-peripheral steepening, which exposes the peripheral retina to myopic defocus throughout the day. Myopic defocus is paramount in slowing axial elongation (Hiraoka, 2022). In fact, ortho-k can slow myopia progression by slowing axial elongation by an average of about 50% (Walline, 2016; Hiraoka et al, 2012; Swarbrick et al, 2015).
Let’s review two key fitting factors to ensure optimal myopia control for patients wearing ortho-k lenses.
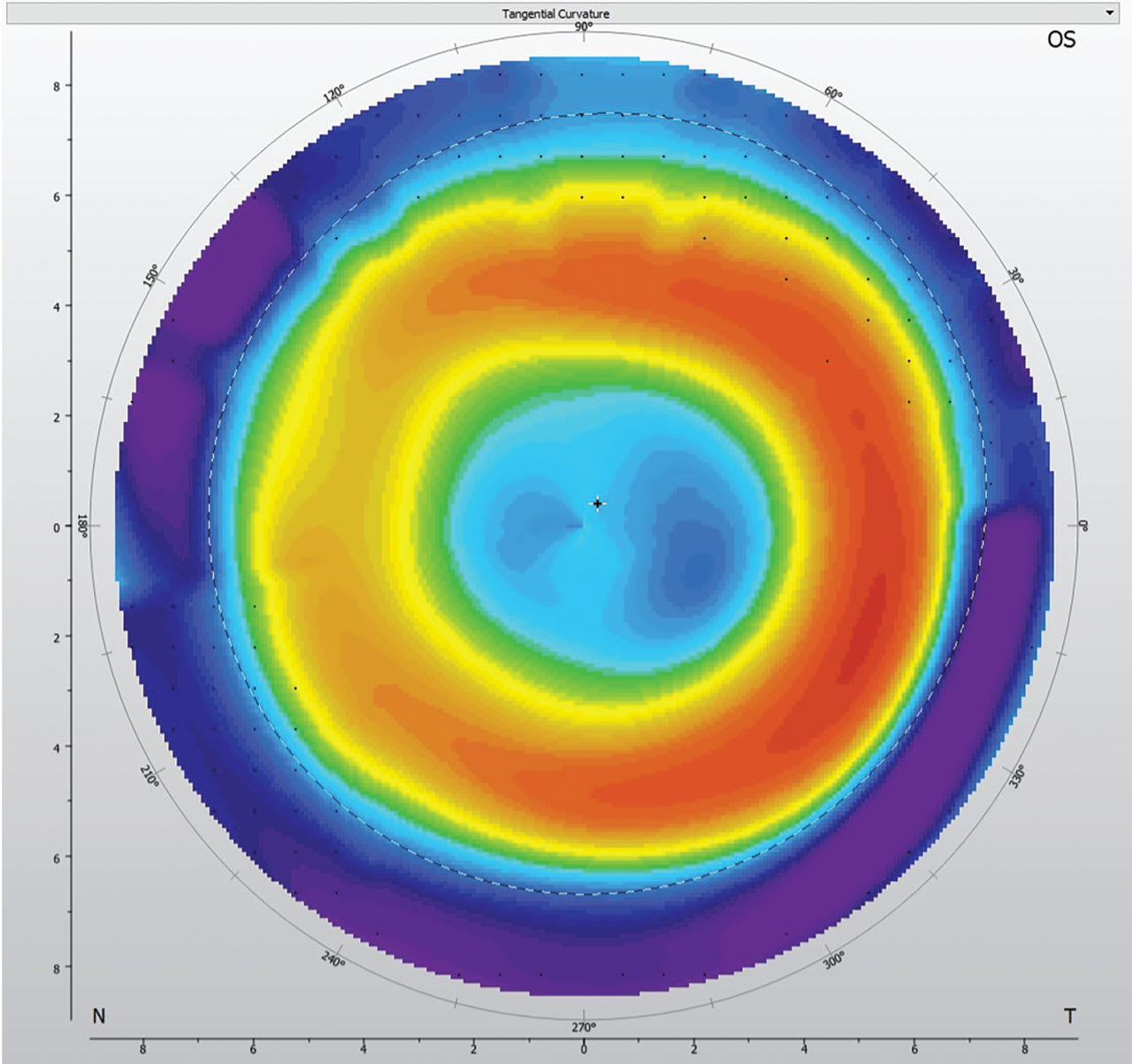
1. Centration The ideal ortho-k lens creates the characteristic bull’s-eye pattern visualized on a topographical map as a red ring surrounding the pupil (Figure 1). Proper lens centration ensures even reshaping of the central cornea and symmetric, mid-peripheral corneal steepening—creating the intended myopic defocus in the peripheral retina. Thus, when the lens is centered, the treatment zone is also centered over the visual axis. In addition, proper lens centration allows the best opportunity for clear, consistent vision throughout the day. On the contrary, a decentered lens may disrupt peripheral myopic defocus, undermining the lens’s effectiveness in slowing myopia progression.
2. Treatment Zone Size The back optic zone diameter (BOZD) of an ortho-k lens directly correlates with the size of the central treatment zone. This specific parameter can be customized based on the patient’s visual needs and desired clinical results. Theoretically, a smaller treatment zone should provide better myopia control due to the increase in peripheral higher-order aberrations and more of the retina receiving myopic defocus. There’s currently evidence demonstrating reduced axial elongation in patients wearing a lens design with a 5mm BOZD versus a 6mm BOZD (Gong et al, 2024). However, each patient should be considered individually, as pupil size and refractive status may dictate the appropriate treatment zone despite the desire for the most effective myopia control.
Lastly, although proper centration and treatment zone are key factors when designing lenses specifically for myopia control, also bear in mind that certain refractive errors provide the best and most predictable clinical results. Low to moderate levels of myopia of –0.50D to –4.50D and up to –1.50D of astigmatism are considered best candidates (Cho and Cheung, 2012; Santodomingo-Rubido et al, 2012; Chen et al, 2013). There are certainly ortho-k designs that can successfully accommodate both higher myopia and astigmatism, but these applications would be considered off-label. In addition, some patients with higher refractive errors may experience reduced vision due to partial correction because of the anatomical restriction of the cornea.
Ortho-k lenses are a fantastic option for patients looking to eliminate daytime vision correction while also benefiting from myopia control. To optimize the patient’s experience, it’s critical to ensure the refractive error is within an acceptable range, the lenses are properly centered, and the treatment zone is appropriately sized.
REFERENCES
1. Hiraoka T. Myopia Control With Orthokeratology: A Review. Eye Contact Lens. 2022 Mar 1;48:100-104.
2. Walline JJ. Myopia Control: A Review. Eye Contact Lens. 2016 Jan;42:3-8.
3. Hiraoka T, Kakita T, Okamoto F, Takahashi H, Oshika T. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up study. Invest Ophthalmol Vis Sci. 2012;53:3913-3919.
4. Swarbrick HA, Alharbi A, Watt K, Lum E, Kang P. Myopia control during orthokeratology lens wear in children using a novel study design. Ophthalmology. 2015;122:620-630.
5. Gong G, Zhang BN, Guo T, et al. Efficacy of orthokeratology lens with the modified small treatment zone on myopia progression and visual quality: a randomized clinical trial. Eye Vis (Lond). 2024 Sep 2;11:35.
6. Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012 Oct 11;53:7077-7085.
7. Santodomingo-Rubido J, Villa-Collar C, Gilmartin B, Gutiérrez-Ortega R. Myopia control with orthokeratology contact lenses in Spain: refractive and biometric changes. Invest Ophthalmol Vis Sci. 2012 Jul 31;53:5060-5065.
8. Chen C, Cheung SW, Cho P. Myopia control using toric orthokeratology (TO-SEE study). Invest Ophthalmol Vis Sci. 2013 Oct 3;54:6510-6517.
