


Marika is a 9-year-old patient referred to me to manage her progressing myopia.The referring professional reported that her myopia began at the age of 6. After she was fit with anti-myopia spectacles, her myopia progression stabilized. At the age of 8, Marika began participating in sporting activities and was refitted with orthokeratology (OK) lenses for myopia control.
Unexpectedly, her myopia began to progress again. The referral was made to reevaluate the case and consideradding low-dose atropine or switching to soft multifocals. In such cases, what would you recommend?
DOCUMENT THE CASE
Myopia management requires an individualized approach. Management should be based on the potential for myopia to progress to more pathological states and on principles generally recognized in the field. The goal is for the myopic child to evolve at the same pace as an emmetropic child of the same age, sex, and ethnic origin.
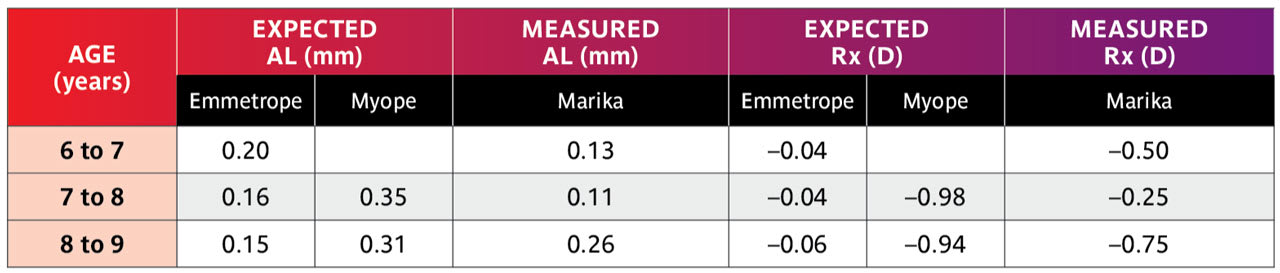
To understand the clinical meaning of this objective for Marika, we looked at the expected progression of an emmetropic Caucasian girl between the ages of 6 and 9 years. Based on Zadnik’s study,1 the expected axial length and refractive error values are shown in Table 1. In order to judge Marika’s progress, we looked at the expected progression of a myope not undergoing myopia management2 (Table 2).


Marika’s first optical correction was initiated at the age of 6. At that time, her refractive error was –1.25 –0.50 x 170 (SE –1.50) OD and –0.75 –0.50 x 020 (SE –1.00) OS with axial lengths of 23.4mm and 23.2mm, respectively. According to the Tideman growth chart,3 Marika was at the 95th percentile with a 16% risk of high myopia in adulthood. It was therefore necessary to develop an effective and intensive strategy to slow down the progression and, if possible, reduce the long-term pathological risk of her myopia.
Marika’s expected versus actual myopic progression is displayed in Table 3. Her myopic condition was relatively well controlled and close to emmetropic progression values during the two years that she wore glasses, but went out of control when she switched to OK lenses.
WHAT OCCURRED?
Myopic progression is influenced by several factors. In Marika’s case, there did not appear to have been any major lifestyle disruptions other than an increase in outdoor physical activity. Time spent outdoors is recognized as a protective factor against the onset of myopia4 in a dose-response modality,5 but not as a contributory factor in slowing myopic progression.6 At the very least, time spent outdoors reduces the amount of time a child spends indoors and can partially reduce the negative impacts of tablet or smartphone use.7
Marika did not have a growth spurt, another factor that can explain myopic progression. She did not change her reading habits (time, reading distance, ambient lighting), knowing that increased near work may contribute to myopia progression.8
With genetic and epigenetic factors stable, we turned our attention to optical correction. The most likely disruption myopic management is noncompliance. It has been shown that noncompliance by people wearing anti-myopia spectacles can lead to rapid myopia progression.9 These spectacles must be worn for more than 10-12 hours a day to be effective.10 Marika’s good compliance during the two years that she wore the glasses appeared to have controlled her myopia progression.
Several factors affect the efficacy of ortho-k lenses, including age, sex, baseline spherical equivalent refraction, keratometry readings, and near-work time.11 The OK lens design, lens centration, and the number of sleeping hours should also be considered. For example, lenses worn for six hours per night or less showed reduced efficacy compared to lenses worn for eight hours.12 Marika’s parents confirmed that their young sportswoman was compliant and wore her OK lenses for an average of nine hours per night.
Clinical assessment revealed that Marika’s uncorrected visual acuity was adequate (20/25 monocularly and 20/20+binocularly). Uncorrected refractive error (myopia, astigmatism) contributing to reduced visual acuity could be likened to form deprivation, and results in a negative retinal signal as bone morphogenetic proteins are downregulated, contributing to eye elongation.13
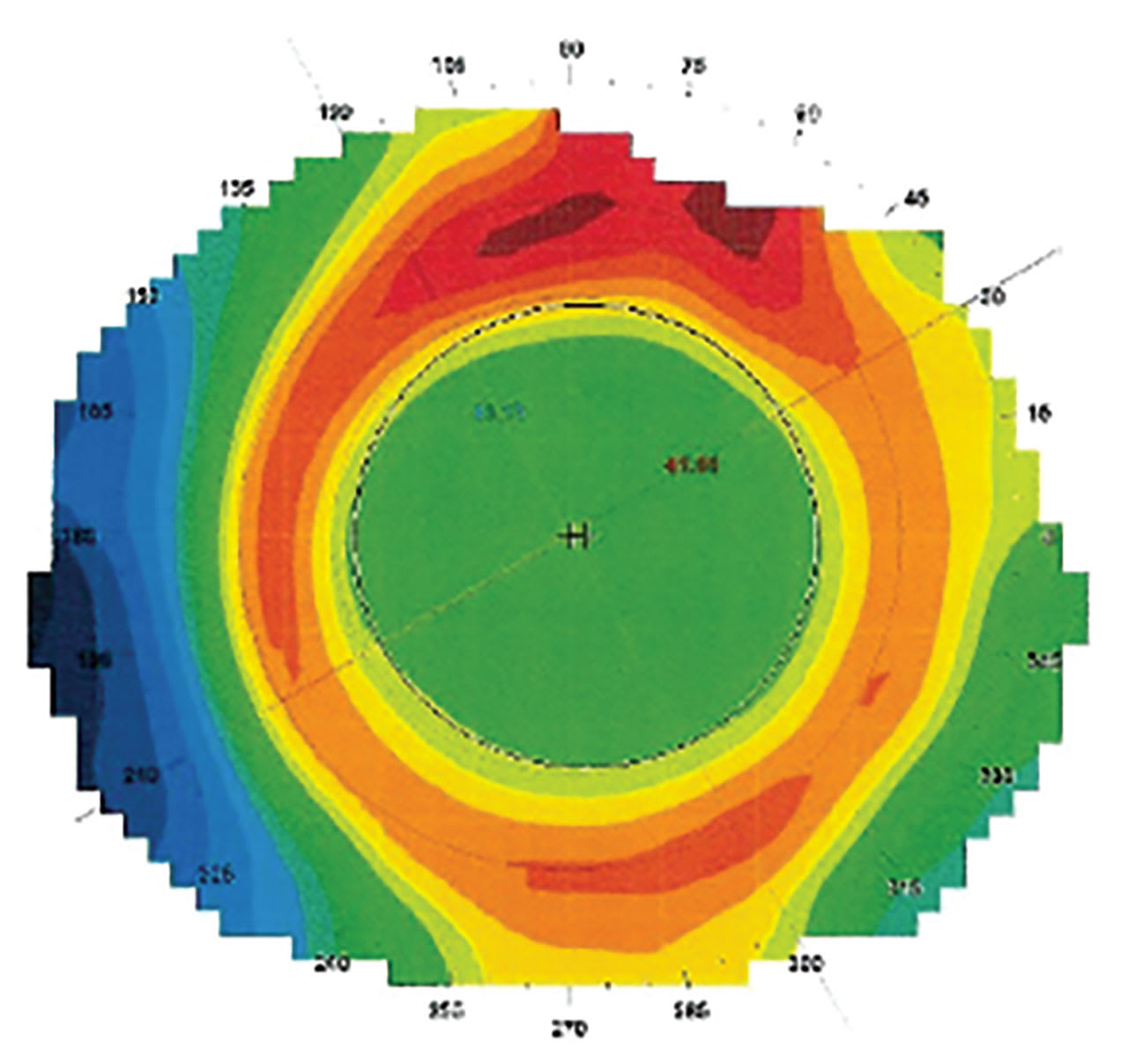
The position of the lens on the eye must be assessed by topography, not under slit lamp examination. When the eyes are open, the lens is subject to gravity. Interaction with the tear film is not the same while blinking as it is with the eye closed. Analysis of the topographer’s tangential map allows us to validate the lens’s behavior and measure its impact on the corneal profile.14 In Marika’s case, the topography showed that the lenses were perfectly centered (Figure 1).
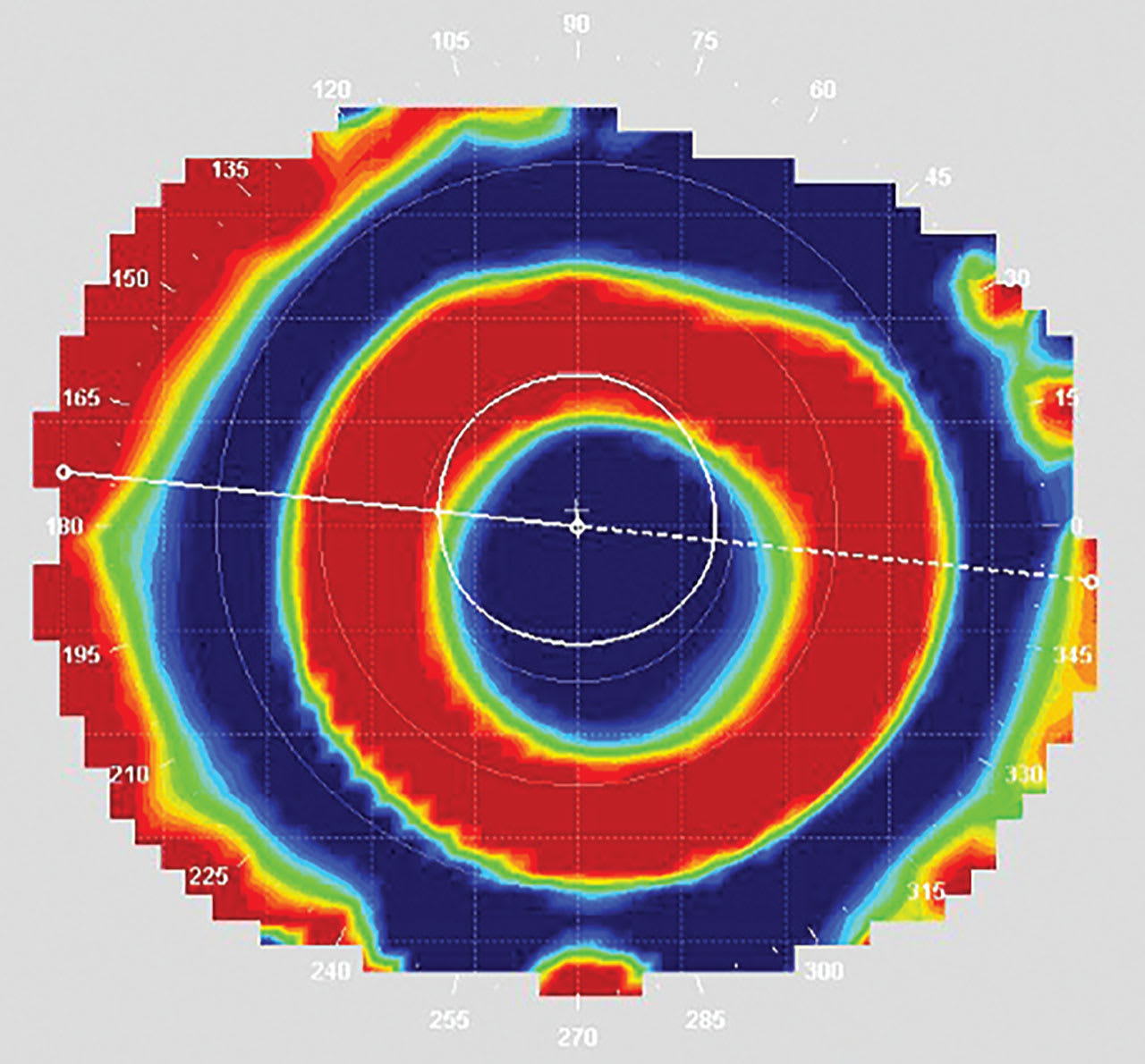
A slightly decentered lens can provide a greater myopia control effect than a perfectly centered lens.15 This counterintuitive conclusion is illustrated by the tangential topography map. A decentered lens moves the more convex powers associated with myopic defocus inside the pupil, thus increasing the “dose” of defocus to which the retina is subjected (Figure 2).
A DOSE-RESPONSE
The retina demonstrates a dose-response16,17 and individual threshold18 to myopic defocus. The greater the myopic defocus, the greater the positive retinal response through a proportional increase in choroidal thickness and resistance to elongation.19
Standard OK lenses generate defocus at a ratio of nearly 1:1.20 Therefore, a lens that corrects a spherical equivalent refraction of –1D will generate approximately +1D of defocus. This is often insufficient, especially for young fast progressors.
The dose delivered is also influenced by the location of defocus on the retina. It is known that the near-peripheral retina is most sensitive to positive defocus between 6º to 10º around the fovea,21 i.e., 1.8mm to 3mm (1º = 0.3mm) in the middle of the macula (average diameter 5.5mm).22 The temporal and inferior quadrants are more reactive based on the response of bipolar and ganglion cells, which suggests a potential feedback loop from the inner to the outer retinal layers to modulate visual signaling and axial elongation.23
THE IMPORTANCE OF THE PUPIL
Does pupil size matter in soft multifocal and OK contact lens fitting for myopia management as it does for presbyopia?24 A recent study compared two soft multifocal contact lens designs for myopia management and found that one performed better in patients who have smaller pupils, while the other performed better in those with larger pupils.25 A separate study examining the effects of pupil size on eye growth found that pupil diameter did not significantly affect axial elongation.26
The pupil delimits which light rays enter the eye. Peripheral paraxial rays transmit defocus to the retinal periphery. Although this is something to consider, it should be remembered that the sensitive zone of the retina is very close to the fovea, as previously mentioned. The defocus must therefore be generated close to the visual axis if it is to reach the correct target. Orthokeratology assumes that the convex power zone is contained within the pupil and not outside it. A smaller treatment zone diameter is consequently favored for greater myopia management efficacy.27
ANATOMY OF AN OK LENS
Modern OK lenses are designed with a reverse-geometry profile and feature four to five curvatures. They are designed to use the hydraulic forces of the post-lens tear film to mold the cornea.28 While it was long believed that these forces caused the migration of epithelial cells, it has now been shown that they cause compression or transfer of fluid (swelling)29 within the epithelial cells to bring about the desired flattening or steepening, respectively.30
The base curve (BC) of the lens is selected according to the refractive error to be corrected. An over-correction known as the Jessen factor is included to account for thereturn of the cornea to its original shape during the day.
Unlike regular GP lenses, OK lenses have a second curve that is steeper than the BC. This allows for the formation of a tear reservoir that induces a negative hydraulic force to steepen the cornea. As a result, refraction through this zone is more convex, creating a myopic defocus. The significant increase in positive spherical aberrations generated directly impacts the quality of the optical signal reaching the retina.31 Coma is added in the event of lens decentration, which also contributes to myopic control.32
The landing zone of an OK lens features one or more curves. This area of the lens is crucial for stability and centration on the eye. When the cornea has an elevation difference of 25 microns or more between the principal meridians at a 8mm chord, it is necessary to use toric rather than spherical peripheral curves for optimal stability and optical effect. 33
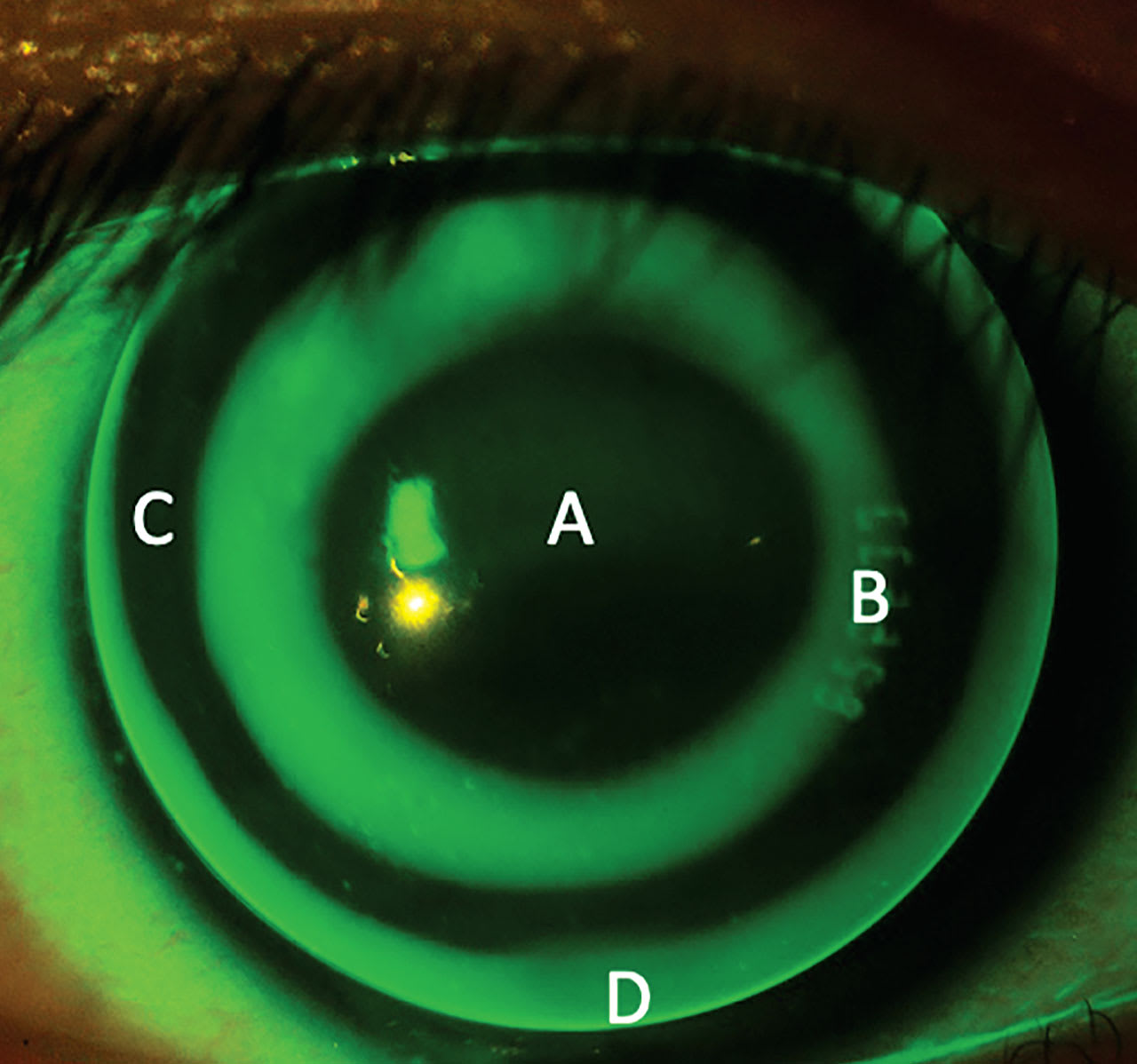
Finally, the peripheral curvature(s) of the OK lens regulate tear exchange (Figure 3).
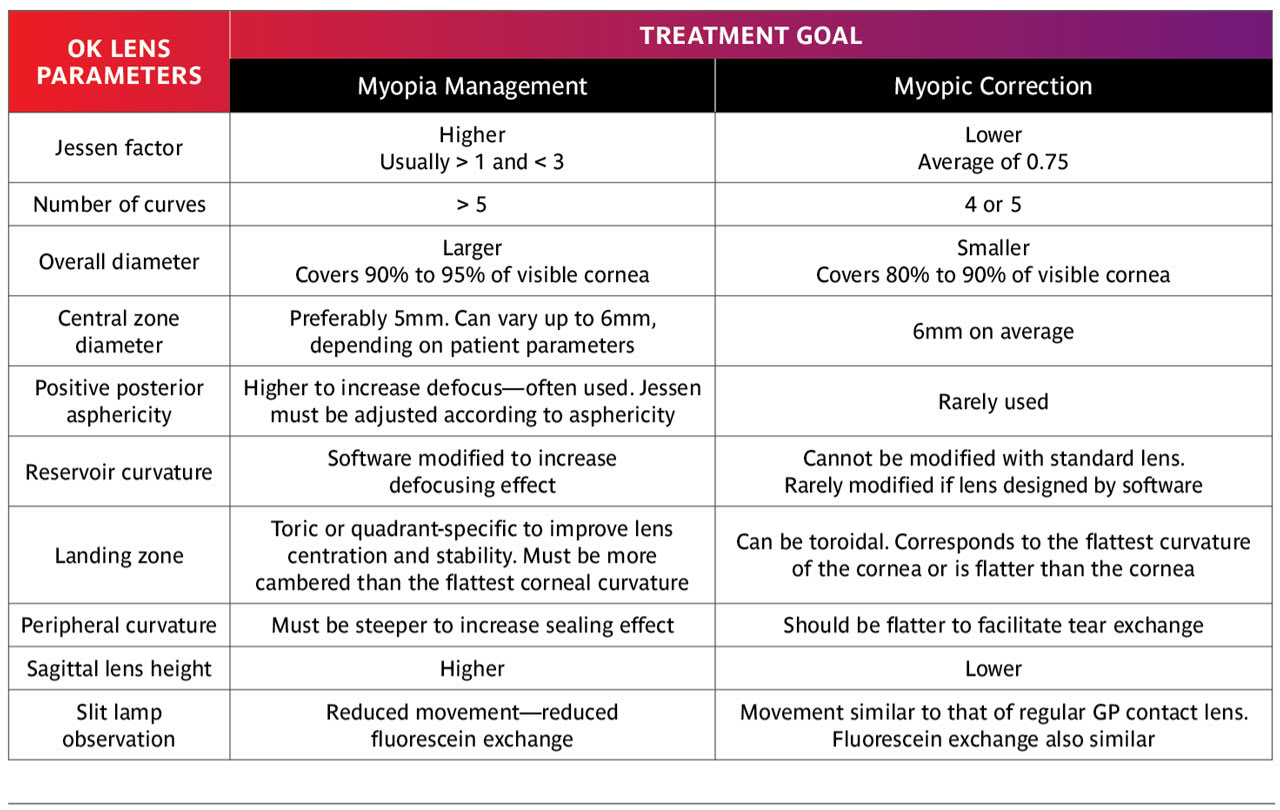
OK FOR MYOPIC CORRECTION OR MYOPIA MANAGEMENT
First, one must consider the goal of treatment. For myopic correction, the goal is to provide optical clarity by correcting refractive error with minimal higher-order aberrations (HOAs). Thus, a large central treatment zone is preferred, and the defocus zone under the reservoir should ideally be as far away from the pupil as possible. These modifications minimize the perception of halos or glare and reductions in contrast sensitivity.
For myopia control, the goal is to slow axial elongation by generating HOAs (spherical aberration and coma) and myopic defocus to affect the optical signal to the retina. Compensation for refractive error is secondary and represents a bonus to the proposed treatment. In this case, a smaller central treatment zone diameter is preferred for greater treatment effect.34,35 Although this reduction in central zone diameter is accompanied by a lower level of convex power in the reservoir, the volume of defocus generated is greater and more effectively slows axial elongation.
It is also possible to increase the level of defocus by adding asphericity to the back surface of the lens.36 This breaks the 1:1 ratio of refractive error correction and defocus discussed above. This is essential when correcting small refractive errors while maximizing the defocus in the system. Indeed, a low myope is usually young, which implies fast evolution, and therefore an increased dose of defocus is required to manage these patients.37
Some practitioners use specialized software to customize OK lens parameters to meet patient needs. These programs can be used to design lenses with complex geometries comprised of more than four or five curves. Reservoir depth can be modulated according to the desired level of defocus. The software can also be used to modify the Jessen factor, particularly in the case of higher prescriptions. A higher Jessen factor has been associated with better myopia control.38The number of peripheral curves and the angle of transition between the landing zone and the reservoir can also be modified to enhance lens stability and comfort.
Lens centration is essential for maintaining clear distance vision and avoiding induced corneal astigmatism. Changes in central zone diameter and base curve should be reserved for optimizing treatment zone and refractive error correction. To improve lens centration, a larger overall lens diameter is required. In general, OK lenses should cover 90% to 95% of the visible corneal surface.39 A larger lens will enhance both lens centration and patient comfort.
Peripheral curves should be designed with a greater sealing effect in myopia management than in myopic correction.40Hydraulic pressure is providing increased corneal molding thus providing better control.
Table 4 summarizes the differences between OK lens designs for myopia management and designs for myopic correction.39,40
AND MARIKA?
Marika was fitted with a standard OK lens. The defocus generated by the lens was positioned almost entirely outside her pupil, reducing the “dose” to which her retina was exposed. After a three-week washout period, new baseline data were acquired for a new software-designed custom lens. After 10 days of wear, the defocus zone covered around 60% of the pupillary area, which appeared to offer the best balance to keep good vision at all distances.41 The patient perceived more halos in the evening but has quickly adapted to this new vision with limited evening activity. After six months, Marika’s axial length showed the expected emmetropic progression, with a slight increase of 0.05mm. Refraction did not change, based on visual acuity once the lens was in place.
CONCLUSION
No single myopia management strategy is clearly superior to the others. Anti-myopia spectacles are generally equivalent to contact lenses or atropine.42 However, the design of each of these optical devices must be optimized, and often customized, for the patient. Adapting the design of OK lenses to improve myopia management appears to be imperative when we analyze recent studies, and especially when cases like Marika’s prove this beyond any doubt.
REFERENCES
1. Zadnik K, Mutti DO, Mitchell GL, Jones LA, Burr D, Moeschberger ML. Normal eye growth in emmetropic schoolchildren. Optom Vis Sci. 2004 Nov;81:819-828.
2. Brennan NA, Shamp W, Maynes E, Cheng X, Bullimore MA. Influence of age and race on axial elongation in myopic children. Optom Vis Sci. 2024 Aug;101:497-507.
3. Tideman JWL, Polling JR, Vingerling JR, et al. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018 Dec;96:301-309.
4. Lingham G, Yazar S, Lucas RM, et al. Time spent outdoors in childhood is associated with reduced risk of myopia as an adult. Sci Rep. 2021 Mar 18;11:6337.
5. Ho CL, Wu WF, Liou YM. Dose-Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods. Int J Environ Res Public Health. 2019 Jul 21;16:2595.
6. Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017 Sep;95:551-566.
7. Enthoven CA, Tideman JWL, Polling JR, Yang-Huang J, Raat H, Klaver CCW. The impact of computer use on myopia development in childhood: The Generation R study. Preventive Medicine. 2020 Mar;132:105988.
8. Karthikeyan SK, Ashwini DL, Priyanka M, Nayak A, Biswas S. Physical activity, time spent outdoors, and near work in relation to myopia prevalence, incidence, and progression: An overview of systematic reviews and meta-analyses. Indian J Ophthalmol. 2022 Mar;70:728-739.
9. Lam CS, Tang WC, Tse DY, Tang YY, To CH. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: a 2-year randomised clinical trial. Br J Ophthalmol. 2014 Jan;98:40-45.
10. Drobe B, Spiegel DP, Yang A, et al. Influence of wearing time on myopia control efficacy of spectacle lenses with aspherical lenslets. Invest Ophthalmol Vis Sci. 2022 Jun;63:4324-A0029.
11. Chen X, Xiong Y, Liu F, Wang J, Yang B, Liu L. Factors determining the myopia control effect of an orthokeratology lens: A two-year multi-level model. Ophthalmic Physiol Opt. 2022 Jul;42:786-796.
12. Zhao W, Wang J, Chen J, et al. The rate of orthokeratology lens use and associated factors in 33,280 children and adolescents with myopia: a cross-sectional study from Shanghai. Eye (Lond). 2023 Oct;37:3263-3270.
13. Zhang Y, Phan E, Wildsoet CF. Retinal Defocus and Form-Deprivation Exposure Duration Affects RPE BMP Gene Expression. Sci Rep. 2019 May 14;9:7332.
14. Tucker A. Topography-Based Fitting Can Improve OrthoK Efficiency. Rev Myopia Management. 2023 Mar 9.
15. Zhang S, Zhang H, Li L, Yang X, Li S, Li X. Effect of treatment zone decentration on axial length growth after orthokeratology. Front Neurosci. 2022 Oct 20;16:986364.
16. Tse DY, To CH. Graded competing regional myopic and hyperopic defocus produce summated emmetropization set points in chick. Invest Ophthalmol Vis Sci. 2011 Oct 17;52:8056-8062.
17. Zhong Y, Chen Z, Xue F, Zhou J, Niu L, Zhou X. Corneal power change is predictive of myopia progression in orthokeratology. Optom Vis Sci. 2014 Apr;91:404-411.
18. Tepelus TC, Schaeffel F. Individual set-point and gain of emmetropization in chickens. Vision Res. 2010 Jan;50:57-64.
19. Wang Z, Chen J, Kang J, Niu T, Guo L, Fan L. Axial Length Control Is Associated With a Choroidal Thickness Increase in Myopic Adolescents After Orthokeratology. Eye Contact Lens. 2023 Dec 1;49:512-520.
20. Queirós A, González-Méijome JM, Jorge J, Villa-Collar C, Gutiérrez AR. Peripheral refraction in myopic patients after orthokeratology. Optom Vis Sci. 2010 May;87:323-329.
21. Swiatczak B, Scholl HPN, Schaeffel F. Retinal “sweet spot” for myopia treatment. Sci Rep. 2024 Nov 5;14:26773.
22. Kolb H. Facts and Figures Concerning the Human Retina. In Kolb H, Fernandez E, Nelson R, eds. Webvision: The Organization of the Retina and Visual System [Internet]. Salt Lake City: University of Utah Health Sciences Center; 1995-.
23. Amorim-de-Sousa A, Pauné J, Silva-Leite S, Fernandes P, Gozález-Méijome JM, Queirós A. Changes in Choroidal Thickness and Retinal Activity with a Myopia Control Contact Lens. J Clin Med. 2023 May 23;12:3618.
24. Bennett ES. Contact lens correction of presbyopia. Clin Exp Optom. 2008 May;91:265-278.
25. De Gracia P, Savla K, Pucker AD. The Impact of Pupil Size on Myopia Control with Multifocal Contact Lenses: A Comparative Study of MYLO and MiSight. Invest Ophthalmol Vis Sci. 2024 Jun;65:2744.
26. Berntsen DA, Ticak A, Sinnott LT, et al. Peripheral Defocus, Pupil Size, and Axial Eye Growth in Children Wearing Soft Multifocal Contact Lenses in the BLINK Study. Invest Ophthalmol Vis Sci. 2023 Nov 1;64:3.
27. Pauné J, Fonts S, Rodríguez L, Queirós A. The Role of Back Optic Zone Diameter in Myopia Control with Orthokeratology Lenses. J Clin Med. 2021 Jan 18;10:336.
28. Vincent SJ, Cho P, Chan KY, et al. BCLA CLEAR - Orthokeratology. Cont Lens Anterior Eye. 2021 Apr;44:240-269.
29. Cheah PS, Norhani M, Bariah MA, Myint M, Lye MS, Azian AL. Histomorphometric profile of the corneal response to short-term reverse-geometry orthokeratology lens wear in primate corneas: a pilot study. Cornea. 2008 May;27:461-470.
30. Choo JD, Caroline PJ, Harlin DD, Papas EB, Holden BA. Morphologic changes in cat epithelium following continuous wear of orthokeratology lenses: a pilot study. Cont Lens Anterior Eye. 2008 Feb;31:29-37.
31. Lian Y, Shen M, Huang S, et al. Corneal reshaping and wavefront aberrations during overnight orthokeratology. Eye Contact Lens. 2014 May;40:161-168.
32. Mathur A, Atchison DA, Charman WN. Myopia and peripheral ocular aberrations. J Vis. 2009 Sep 21;9:15.1-12
33. Kojima R, Caroline P, Morrison S, et al. Should all orthokeratology lenses be toric? Poster presented at the Global Specialty Lens Symposium, Jan. 21-24, 2016; Las Vegas.
34. Guo B, Cheung SW, Kojima R, Cho P. One-year results of the Variation of Orthokeratology Lens Treatment Zone (VOLTZ) Study: a prospective randomised clinical trial. Ophthalmic Physiol Opt. 2021 Jul;41:702-714.
35. Tang WT, Luo XN, Zhao WJ, et al. One-year results for myopia control of orthokeratology with different back optic zone diameters: a randomized trial using a novel multispectral-based topographer. Int J Ophthalmol. 2024 Feb 18;17:324-330.
36. Herzberg C. 10 Tips from an Orthokeratology Expert. Rev Cornea Cont Lens. 2017 Feb 15.
37. Lau JK, Wan K, Cho P. Orthokeratology lenses with increased compression factor (OKIC): A 2-year longitudinal clinical trial for myopia control. Cont Lens Anterior Eye. 2023 Feb;46:101745.
38. Michaud L, Simard P, Marcotte-Collard R, Ouzzani M. Managing myopia: one child at a time. Toronto: Dougmar Publishers; 2022.
39. Michaud L, Simard P. Myopia Conterol with Ortho-k. Contact Lens Spectrum. 2017 Sep;32:20-26.
40. Lu W, Ning R, Diao K, et al. Comparison of Two Main Orthokeratology Lens Designs in Efficacy and Safety for Myopia Control. Front Med (Lausanne). 2022 Apr 1;9:798314.
41. Rio D, Legras R. Which ratio of areas improves vision quality in simultaneous focus optics? Optom Vis Sci. 2015 Apr;92:429-436.
42.Lanca C, Pang CP, Grzybowski A. Effectiveness of myopia control interventions: A systematic review of 12 randomized control trials published between 2019 and 2021. Front Public Health. 2023 Mar 23;11:1125000.